
Characteristics and uses of IT knife nano
 0
0 ,
, Abstract
IT knife nano® (Olympus Medical Co., Tokyo, Japan) is a knife device specialized for esophageal and colorectal endoscopic submucosal dissection (ESD). The IT knife nano has a smaller insulated tip than that of the IT knife 2, making it easier to handle the submucosal layer in the colorectum. The disk behind the insulated tip is also smaller to reduce thermal damage to the muscle layer. Furthermore, the IT knife nano is considered to have more power for incision because the IT knife nano has a large amount of electric current at the blade compared to other devices. Therefore, the IT knife nano can resect a larger amount of submucosal layer tissue at once, enabling a faster and more reliable detachment of the submucosal dissection as well as a circumferential mucosal incision. When performing submucosal dissection using an IT knife nano, the knife should be moved from the outside to the inside. While in a difficult situation, moving the knife gradually from the center (inside) to the outside can help perform a safe colorectal ESD. The IT knife nano is considered an option for difficult situations, such as lesions with severe fibrosis, or when rapid submucosal dissection is required. We herein provided technical aspects of the IT knife nano in detail and compared it with other needle-type devices.
Keywords
INTRODUCTION
Hosokawa et al.[1] and Ono et al.[2] originally developed the IT knife® (Olympus Medical Co., Tokyo, Japan) to perform gastric endoscopic submucosal dissection (ESD) more safely and more effectively compared to the needle-type devices. Subsequently, the IT knife nano® (Olympus Medical Co., Tokyo, Japan), specialized for esophageal and colorectal ESD, was developed by Ono and Yamaguchi. The IT knife nano has a smaller insulated tip, making it easier to handle the submucosal layer. The disk behind the insulated tip is also smaller to reduce thermal damage to the muscle layer. Many studies on colorectal ESD using IT knife nano have been reported[3-5].
CHARACTERISTICS OF IT KNIFE NANO
The IT knife nano can make incisions and resect using an electric current at the blade, one of the unique features that separate it from the needle-type knives. A long blade of IT knife nano makes it possible to resect the connected tissue, which is in contact with the submucosal tissue to be dissected. The IT knife nano is considered to have more power for incision, resection, and coagulation than needle-type devices. This is because the IT knife nano has a large amount of electric current at the blade compared to other devices. However, needle-type devices concentrate the current energy at the top of the needle to increase the current density. Therefore, the IT knife nano can resect a larger amount of submucosal layer tissue at once, enabling a faster[6] and more reliable detachment of the submucosal dissection.
STRUCTURE OF IT-KNIFE NANO
The IT-knife nano has an insulated tip of the blade. A small disk is equipped behind the insulated tip to increase the resection efficiency. This disk makes it possible for the IT knife nano to resect the submucosal layer using the back of the disk touching the connective tissue. However, it should be noted that damage to the muscle layer by the burn effect of the disk may occur when the distance between the disk and the muscle layer is close [Figure 1].
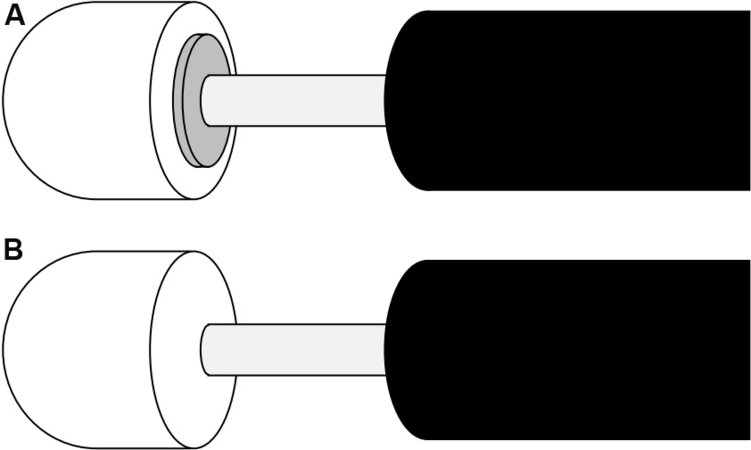
Figure 1. IT knife nano® with and without disk back of an insulated tip. (A) IT knife nano with a disk. A small disc is placed behind the insulated tip. (B) IT knife nano without disk. Only a blade is used for the submucosal dissection.
Therefore, we have used another version of the IT knife nano without a disk to resolve this issue. We used a special made-to-order IT knife nano without a disk for lesions with a narrow submucosal layer caused by fibrosis. This increases the electric current density and improves the resection ability of the blade. This device also makes it easier to slip into the submucosal layer and approach the blade to the submucosal tissue for resection, even if the surgical field is difficult due to fibrosis or other reasons. In addition, an insulated tip without a disk is suitable for resection in a narrow working space of the submucosa. To use a special made-to-order IT knife nano without a disk, requirements have to be met as follows: (1) expert endoscopists perform many colorectal ESDs in a tertiary center; and (2) many IT knife nanos (normal type) are used for colorectal ESD in the hospital. When a hospital matches these criteria, the hospital can order a specially made IT knife nano from the industry.
TECHNIQUES OF IT KNIFE NANO
The IT knife nano is mainly designed to be pulled for resection, whereas other needle-type devices are based on cutting in the pushing direction.
Therefore, when performing submucosal dissection using an IT knife nano, the knife should be moved from the outside to the inside [Figure 2].
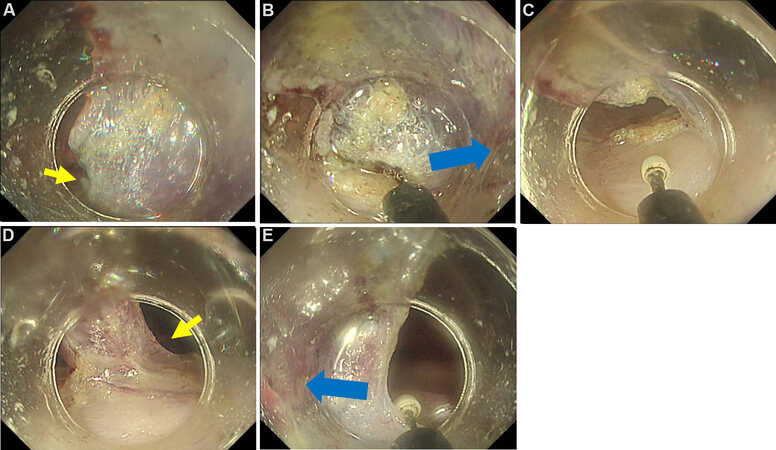
Figure 2. Submucosal dissection using IT knife nano®. (A) The edge of submucosal tissue is recognized using the ST hood short type®. (B, C) The blade of the IT knife nano approaches to the submucosal tissue. Then moving along the muscle layer (blue arrows), submucosal dissection is performed safely. (A, D, E) The procedure is performed turn by turn in both sides (yellow arrows).
The detailed technique is as follows:
First, the edge of the submucosal tissue is visualized, and the knife blade hooked onto that edge. Then, the scope is manipulated along the running of the muscle layer to resect the submucosal tissue. The moving knife direction then should be aimed at the middle of the submucosal layer, which has been raised and thickened by submucosal injection [Figure 3]. Next, submucosal dissection should be performed equally from both sides. It is better to check the direction of resection every two to three times of energizing. In addition, even in cases with relatively large vessels, a longer coagulation wave can be applied to resection without bleeding [Figure 4]. Moving or pushing up the lesions half resected using a sheath of IT knife nano is sometimes effective when the operation field is difficult to recognize. In addition, the ST hood short type® (Fujifilm Co, Tokyo, Japan) is also useful for maintaining the surgical field and a better direct view by pushing up the lesions and their submucosa[5]. Therefore, combining these techniques is one of the keys to safe and effective colorectal ESD using the IT knife nano.
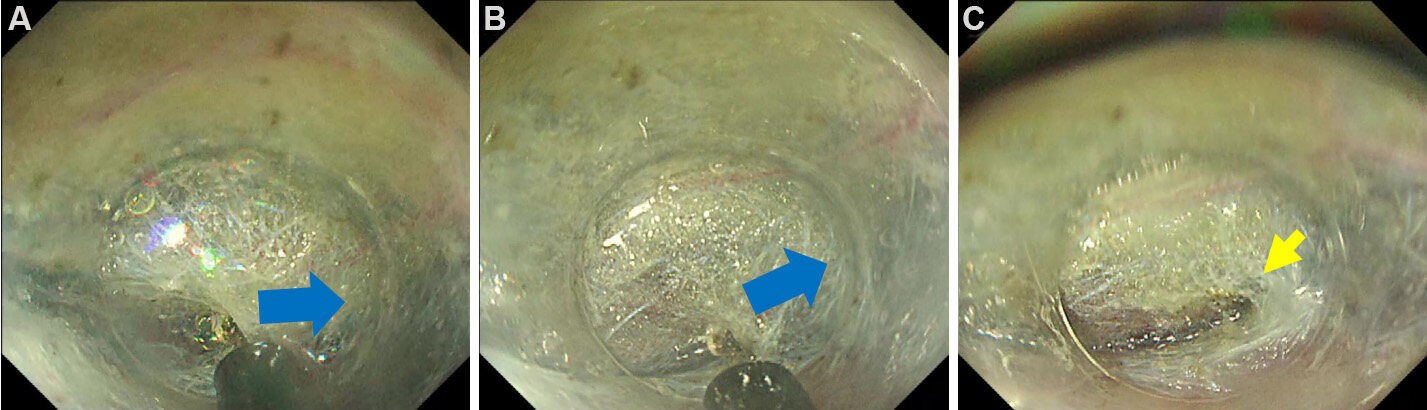
Figure 3. Submucosal dissection using IT knife nano®. (A, B) The blade is hooked in the edge of the submucosal tissue and moving to the center of submucosal layer (blue arrows) injected by blue-colored solution. (C) Submucosal tissue is resected safely (yellow arrow).
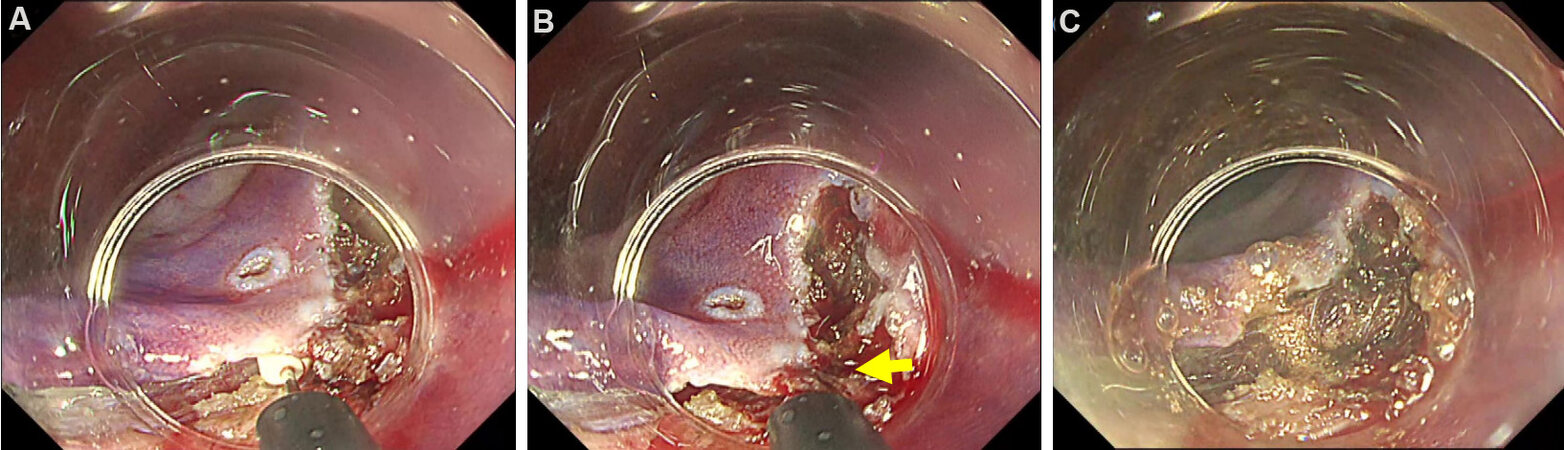
Figure 4. IT knife nano® can resect vessels without coagulation forceps. (A, B) A relatively large vessel is stuck (yellow arrow). (C) Long coagulation wave can burn and resect the tissue and vessel without bleeding.
In some cases, it may be difficult to manipulate the endoscope for anatomical reasons, such as flexure or movement of the lumen by breathing. Alternatively, the operation field of view may be difficult to maintain, and resection should be performed partially blind in such patients. These situations are dangerous. In such cases, moving the knife gradually from the center (inside) to the outside helps perform safe ESD.
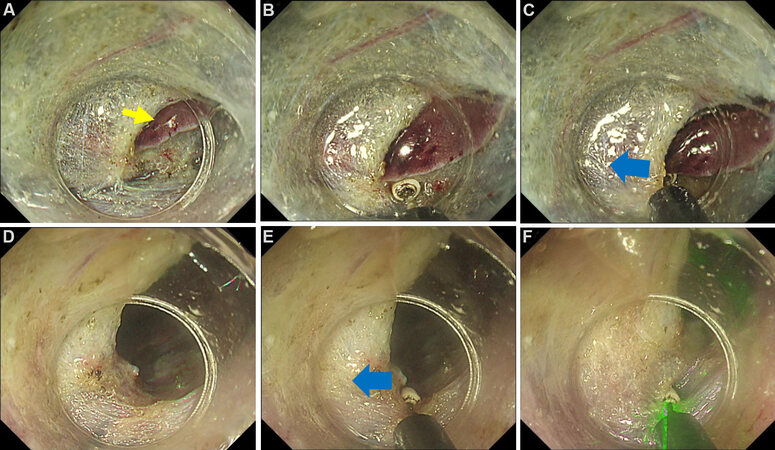
Figure 5. Pocket creation method technique using IT knife nano. (A) An injected submucosal layer is recognized by attaching hood devices. The insulated tip is put at the center of the submucosal layer (yellow arrow). (B, C) A little electric current makes a small indentation. (D-F) After hooking the blade to the edge of the indentation, the IT knife nano can move to the right side slowly (blue arrows) and resect the submucosal layer safely.
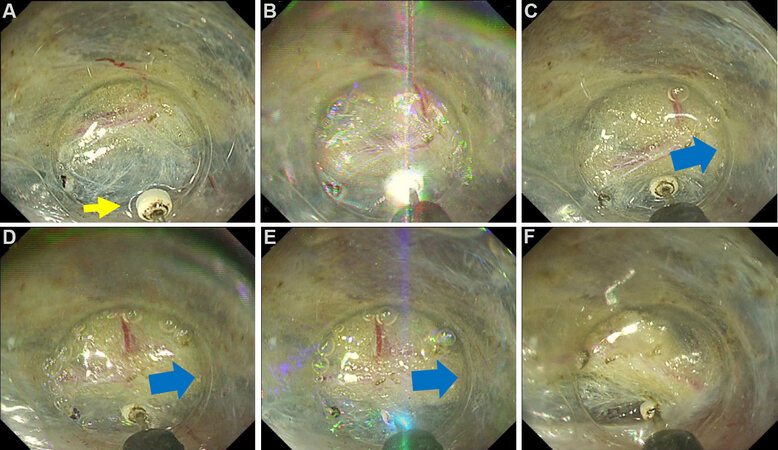
Figure 6. Pocket creation method (PCM) with tunneling technique with IT knife nano®. (A) A tunnel is made after continuing submucosal dissection by PCM (yellow arrow). (B, C) The blade of the IT knife nano is put on the edge of the tunnel and moved a little to the outside (blue arrow). (D-F) The procedure is performed repeatedly (direction to the blue arrow), and submucosal tissue is resected safely even if fibrosis exists.
Another unique use of the IT knife nano is touching the insulated tip to the submucosal tissue to stabilize the endoscope. Then, the submucosal layer can be resected by slowly moving or tilting the blade of the IT knife nano. It is often useful when the endoscope is unstable.
Table 1 lists the devices and settings used in the facility. The generator used was a VIO 300D® or VIO3® (Erbe Elektromedizin, Tuebingen, Germany). We used three coagulation modes, depending on the situation in VIO3.
Setting of generators for IT knife nano®
| VIO 300D® | Cut mode | Coagulation mode | ||
| Effect | 3 | 2 | ||
| Maximum watt | 100 W | 50 W | ||
| VIO3® | Cut | Coagulation | Coagulation | Coagulation |
| Mode | Dry CUT | Precise SECT | Forced COAG | Swift COAG |
| Effect | 4.7 | 6.0 | 6.0 | 5.0 |
DISCUSSION
Various types of knife devices have been developed for colorectal endoscopic submucosal dissection. Therefore, it is often difficult to choose the optimal type of device. These two points can be considered when selecting a device: choosing the appropriate devices for the situation of colorectal ESD, and using a familiar knife as the main device because colorectal ESD requires training.
When the IT knife nano is used for colorectal ESD, it is mainly used for submucosal dissection. Additional needle-type devices are always required for first incisions. Therefore, performing ESD with a needle-type device should only be considered when cost-effectiveness is emphasized. However, the IT knife nano is considered as an option for difficult situations, such as lesions with severe fibrosis, or when rapid submucosal dissection is required.
CONCLUSION
When choosing a knife with an emphasis on cost-effectiveness, a needle-type knife device seems to be the most appropriate choice. However, the IT knife nano is stable even in situations where luminal movement by breathing or heartbeats make it difficult to use needle-type devices. In addition, it is expected to be able to complete the procedure without hemostatic forceps in colorectal ESD using the IT knife nano because it has superior hemostatic performance compared to the needle-type devices.
The IT knife nano is different from the other needle-type devices in that it does not have a jet function. In the future, it is expected to have more functions as technology progresses and develops. We believe that the IT knife nano is an indispensable device for colorectal ESD in terms of safety, reliability, and efficacy.
DECLARATIONS
Authors’ contributionsData acquisition and writing manuscript: Takamaru H
Made substantial contributions to conception, data acquisition, and supervised: Saito Y
Availability of data and materialsNot applicable.
Financial support and sponsorshipThis work was supported in part by the National Cancer Center Research and Development Fund (25-A-12, 28-K-1, and 29-A-13) to Saito Y.
Conflicts of interestSaito Y received speaker’s fees from Olympus Medical Co., Tokyo, Japan. Takamaru H declared that there are no conflicts of interest.
Ethical approval and consent to participateNot applicable.
Consent for publicationNot applicable.
Copyright© The Author(s) 2022.
REFERENCES
1. Hosokawa K, Yoshida S. Recent advances in endoscopic mucosal resection for early gastric cancer. Gan To Kagaku Ryoho 1998;25:476-83.
2. Ono H, Kondo H, Gotoda T, et al. Endoscopic mucosal resection for treatment of early gastric cancer. Gut 2001;48:225-9.
3. Saito Y, Uraoka T, Matsuda T, et al. Endoscopic treatment of large superficial colorectal tumors: a case series of 200 endoscopic submucosal dissections (with video). Gastrointest Endosc 2007;66:966-73.
4. Saito Y, Uraoka T, Yamaguchi Y, et al. A prospective, multicenter study of 1111 colorectal endoscopic submucosal dissections (with video). Gastrointest Endosc 2010;72:1217-25.
5. Saito Y, Otake Y, Sakamoto T, et al. Indications for and technical aspects of colorectal endoscopic submucosal dissection. Gut Liver 2013;7:263-9.
6. Hotta K, Yamaguchi Y, Saito Y, Takao T, Ono H. Current opinions for endoscopic submucosal dissection for colorectal tumors from our experiences: indications, technical aspects and complications. Dig Endosc 2012;24 Suppl 1:110-6.
Cite This Article
Export citation file: BibTeX | RIS
OAE Style
Takamaru H, Saito Y. Characteristics and uses of IT knife nano. Mini-invasive Surg 2022;6:15. http://dx.doi.org/10.20517/2574-1225.2021.120
AMA Style
Takamaru H, Saito Y. Characteristics and uses of IT knife nano. Mini-invasive Surgery. 2022; 6: 15. http://dx.doi.org/10.20517/2574-1225.2021.120
Chicago/Turabian Style
Takamaru, Hiroyuki, Yutaka Saito. 2022. "Characteristics and uses of IT knife nano" Mini-invasive Surgery. 6: 15. http://dx.doi.org/10.20517/2574-1225.2021.120
ACS Style
Takamaru, H.; Saito Y. Characteristics and uses of IT knife nano. Mini-invasive. Surg. 2022, 6, 15. http://dx.doi.org/10.20517/2574-1225.2021.120
About This Article
Special Issue
Copyright

Data & Comments
Data
0

 Cite This Article 4 clicks
Cite This Article 4 clicks

 Like This Article 0
likes
Like This Article 0
likes






Comments
Comments must be written in English. Spam, offensive content, impersonation, and private information will not be permitted. If any comment is reported and identified as inappropriate content by OAE staff, the comment will be removed without notice. If you have any queries or need any help, please contact us at support@oaepublish.com.