
SB Knife Jr: characteristics and tips on how to use

Abstract
Widespread adoption of colorectal endoscopic submucosal dissection (ESD) in clinical practice is lagging despite the peer evidence that it permits en bloc resection of large lesions that can be curative and facilitate pathological staging, thereby improving management. Limited adoption of colorectal ESD is likely due to technical challenges and a steep learning curve. Most conventional ESD devices are used without fixing the target, making them difficult to maneuver and thus creating a potential risk of perforation. Comparatively, a scissor-type knife, such as the SB Knife Jr, enables grasping of the target tissue, facilitating controlled dissection of tissue being held between the blades. This potentially prevents unexpected muscular layer injury. Colorectal ESD with the SB Knife Jr does not require complex endoscopic maneuvering or advanced skills for safe ESD. Since the incision and dissection procedure using the SB Knife Jr is different from that of conventional ESD knives, familiarization with its features is vital. In this review, we focus on the use of the SB Knife Jr for colorectal ESD. The basic colorectal ESD procedure using the SB Knife Jr consists of grasping, pulling, and cutting. By repeating these steps, circumferential incision, submucosal dissection, and hemostasis can be performed with a single device. For incision and dissection, a circumferential mucosal incision is performed similar to “cutting paper”. Submucosal dissection is performed with the image of “connecting the dots at the appropriate dissection depth”. The SB Knife Jr is useful as a secondary device in challenging ESD procedures, and surgeons should master its use.
Keywords
INTRODUCTION
The advantages of endoscopic submucosal dissection (ESD) include the ability to control resection size and shape and permit en bloc resection of large lesions[1,2]. However, the adoption of colorectal ESD is not widespread because of technical challenges imposed by the complex anatomic features of the large intestine[3]. To overcome these issues, several ESD devices, including the Dual knife, Flex-knife, insulated tipped knife (IT-Knife), Hook-knife (Olympus, Tokyo, Japan), and Flush-knife (Fujifilm, Tokyo, Japan), have been developed over the past two decades for colorectal ESD[4]. Most conventional ESD devices have freehand tips and are used without fixing the target, creating a potential risk of unexpected incision and perforation of the colorectal wall.
In comparison, a scissor-type knife, such as the Stag Beetle Knife Jr (SB Knife Jr, Sumitomo Bakelite, Tokyo, Japan), enables grasping of the target tissue, allowing controlled endoscopic dissection that potentially prevents unexpected muscular layer injury[5]. However, the scissor-type knife has features different from those of other conventional ESD knives. Therefore, in this review, we describe the characteristics of the scissor-type knife, specifically the SB Knife Jr, and discuss how to effectively use it for colorectal ESD.
CHARACTERISTICS OF THE SB KNIFE JR
The SB Knife series
The SB Knife series are scissor-type knives designed to grasp and cut the tissue being held using a monopolar frequency applied through insulated blades (to prevent coagulation of the muscle layer) such that only the tissue grasped within the electrodes is cauterized[6]. There are four types of SB Knife: SB Knife Short, SB Knife GX, SB Knife Jr, and SB Knife Jr 2. Figure 1 shows detailed characteristics of these knives. The SB Knife Short and SB GX have curved blades to prevent coagulation of the muscle layer, whereas the SB Knife GX has a partially serrated edge to prevent tissue slipping. The SB Knife GX is generally used for gastric ESD, the SB Knife Short is used for submucosal dissection in esophageal ESD, and the SB Knife Jr and Jr 2 are developed and used for colorectal and esophageal ESD[5,7-9].

Figure 1. The SB Knife series.
The SB Knife Jr
The SB Knife Jr was launched in 2010[10,11]. Regarding the structure of the SB Knife Jr, the small tapered and curved tip design with superior rotation allows accurate manipulation within the endoscope visual field to minimize unintentional muscular layer injury. This knife has an opening width of 4.5 mm and a length of 3.5 mm.
The SB Knife Jr 2
The newly developed SB Knife Jr (SB Knife Jr 2) was launched in 2019 and is available only in Japan[12]. Figure 2 shows the three major points of improvement of the SB Knife Jr 2. First, the new coating materials improve the coating durability, insulation coating, and incision ability. There is also improved tissue grasping ability because of the new blade design with protrusions. Moreover, a new rotation handle prevents the connection cord from tangling and enables easy manipulation. These improvements are expected to shorten procedure times.
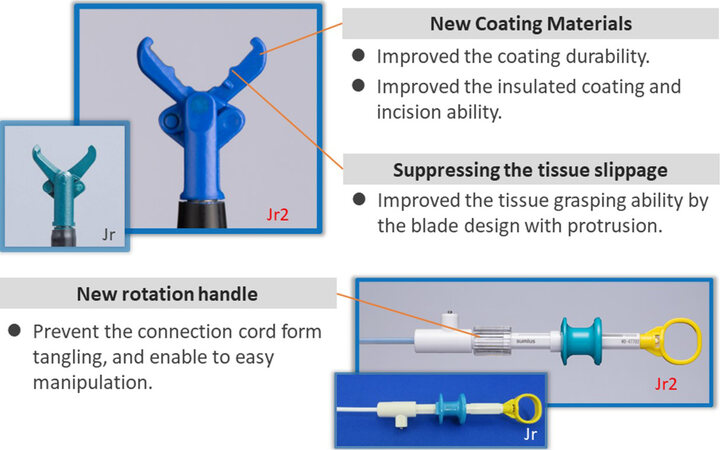
Figure 2. The points of improvement with the SB Knife Jr 2.
Equipment for colorectal ESD using the SB Knife Jr (i.e., high-frequency generator, injection liquid, and tip hood)
The dissected segment is grasped, and a current is passed using a high-frequency generator [VIO300D, VIO3 (ERBE, Tubingen, Germany) or ESG 100 (Olympus)]. The settings for high-frequency generators in colorectal ESD using the SB Knife Jr or Jr 2 at our center are shown in Table 1.
The settings for high-frequency generators in colorectal ESD using the SB Knife Jr or Jr 2 at our center
| Knife | High-frequency generator | Procedure | Setting | ||||
| Mode | Effect | Duration | Interval | Watt | |||
| SB Knife Jr | VIO300D | Mucosal incision/submucosal dissection | Endocut Q | 1 | 1-3 | 1 | - |
| Hemostasis | Soft Coag | 5 | - | - | 40 W | ||
| SB Knife Jr and Jr 2 | ESG-100 | Mucosal incision/submucosal dissection | Pulse Cut First | - | - | - | 30 W |
| Hemostasis | Soft Coag | - | - | - | 40 W | ||
| SB Knife Jr 2 | VIO 3 | Mucosal incision/submucosal dissection | Endocut I | 2 | 3 | 1 | - |
| Hemostasis | Soft Coag | 6.0 | - | - | 40 W | ||
A transparent tip hood (Elastic Touch; Top, Tokyo, Japan) is always used to facilitate traction application on the mucosa when creating space for submucosal dissection with carbon dioxide insufflation. Sodium hyaluronate solution (0.4%; Muco Up; Johnson & Johnson, New Brunswick, NJ, USA) with 0.5 mL of indigo carmine and 0.1 mg of epinephrine is injected into the submucosal layer using a 21-gauge injection needle. It might be useful to have a traction device (such as an S-O clip; Zeon Medical Co., Tokyo, Japan) as well, if needed.
TIPS ON HOW TO USE THE SB KNIFE JR FOR COLORECTAL ESD
Colorectal ESD using the SB Knife Jr does not require simultaneous complex endoscopic movement while applying an electric current; therefore, it can be performed relatively safely and easily. However, the fundamental operating technique is quite different from conventional knives (i.e., needle-type knives). Therefore, it is necessary to be familiar with the characteristics of the SB Knife Jr for colorectal ESD.
Treatment strategy of colorectal ESD using the SB Knife Jr
The endoscopic position during the procedure is kept in a forward view, not using a retroflexed position, and then a circumferential incision and dissection are performed from the anal side[5]. In cases with a large lesion, a proximal incision is made to define the end and guide the circumferential incision. Following that, the treatment strategy of colorectal ESD using the SB Knife Jr is the same as that using conventional knives, such as the mucosal-flap method, tunneling method, and pocket-creation method.
The following are some useful tips for incision and dissection using the SB Knife Jr: perform the circumferential mucosal incision similar to cutting paper and the submucosal dissection the image of “connecting the dots at the appropriate dissection depth”[13]. The basic colorectal ESD procedure using the SB Knife Jr consists of the following three steps, and a circumferential incision, submucosal dissection, and hemostasis can all be performed using a single device.
The three basic steps for ESD procedure using the SB Knife Jr [Figure 3]
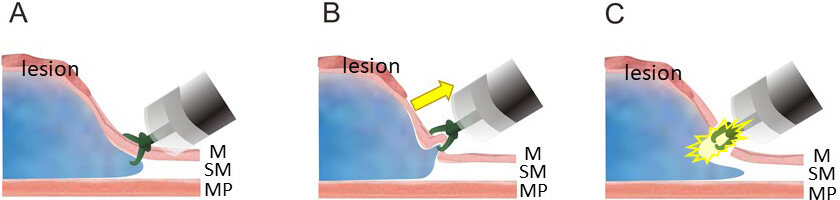
Figure 3. The three basic steps of the ESD procedure using the SB Knife Jr: (A) grasping; (B) pulling; and (C) cutting. ESD: Endoscopic submucosal dissection.
Step 1: grasping
The target tissue is approached and grasped with the SB Knife Jr as in the biopsy technique. Inadvertent resection can be avoided by regrasping, which ensures safety. In the case of severe fibrosis of the target tissue, the scissors are closed slowly to facilitate grasping. In situations wherein it is difficult to manipulate the scope, the scope position should be fixed while simply inserting and pulling the SB Knife Jr (not moving the scope, moving the knife only). With more experience, the endoscopist can control the opening of the knife to open slightly to grasp even single-strand fibers.
Step 2: pulling
The safety of the ESD procedure can be ensured by pulling the SB Knife Jr slightly forward and away from the muscle layer while grasping the target tissue to avoid electrical damage to the muscle layer. With experience and when the lesion is sufficiently elevated by submucosal injection, it becomes possible to skip the pulling step and move on to the third step of cutting the grasped tissue using an electric current, which can speed up the procedure considerably.
Step 3: cutting
After confirming that the SB Knife Jr does not grasp the muscle layer together, the cutting electric current is applied, and the grasped tissue is incised. Even if there are small blood vessels within the tissue, intraoperative bleeding usually does not occur. However, if the tissue contains large blood vessels, applying the coagulation electric current as prophylactic hemostasis for about 1 s twice before attempting incision prevents bleeding.
Hemostasis procedure using the SB Knife Jr
The hemostasis procedure using the SB Knife Jr also follows the three steps described above, almost the same as when using hemostatic forceps. Grasp a bleeding vessel precisely; pull the grasped vessel slightly (or skip this step if far from the muscle layer); and apply the coagulation electric current for approximately 1 s two or three times. Most cases can be managed with this procedure; however, if hemostasis is not achieved after two or three attempts using the SB Knife Jr, the device can be changed to hemostatic forceps (e.g., Coagraspar; Olympus, Tokyo, Japan).
ADVANTAGES AND DISADVANTAGE OF THE SB KNIFE JR FOR COLORECTAL ESD
The technique of colorectal ESD using the SB Knife Jr is the same as that for the biopsy technique, which does not require advanced skill and complex endoscopic manipulation. The rate of ESD self-completion for trainees was reported as significantly better with the SB Knife Jr than with a needle-type knife[14]. Additionally, it is safe because the electric current can be applied just after confirming that the SB Knife Jr did not grasp the muscle layer[15]. As the SB Knife Jr also works as hemostasis forceps, there is no need to change the device in the case of intraoperative bleeding during the procedure. This might be more cost-effective because hemostasis forceps are not needed[16]. These advantages of the SB Knife Jr make it useful not only for trainees but also for experts in difficult situations.
A few reported disadvantages of the SB Knife Jr are prolonged procedure time of ESD as its use requires multiple steps, as stated above[5,17]. In addition, the training of an assistant is needed to teach them how to rotate the knife because effective knife rotation technique by assistants is essential in colorectal ESD when using the SB Knife Jr[18]. Another contributing factor for a prolonged procedure time may include the fact that the SB Knife Jr lacks water-jet function, which is reportedly effective for reducing the procedure time of colorectal ESD[19].
These disadvantages have been overcome with the development of the new SB Knife Jr 2. This new knife is equipped with a rotation handle for one-to-one rotation of blades that facilitate easy manipulation by an assistant. New coating materials to prevent unnecessary diathermy burn and a new blade design with a protrusion might contribute to speedier resection[12]. In addition, traction devices (such as an S-O clip) significantly reduce the procedure time in colorectal ESD using scissor-type knives[15,20].
CASE PRESENTATION OF COLORECTAL ESD USING SB KNIFE JR [Supplementary Video1]
A 61-year-old man was referred to our center with a 0-IIa (LST-NG) lesion of 40 mm in size at the transverse colon [Figure 4A and B]. Magnifying endoscopic observation revealed a JNET 2 B and Vi (high-grade) pit pattern lesion [Figure 4C and D].
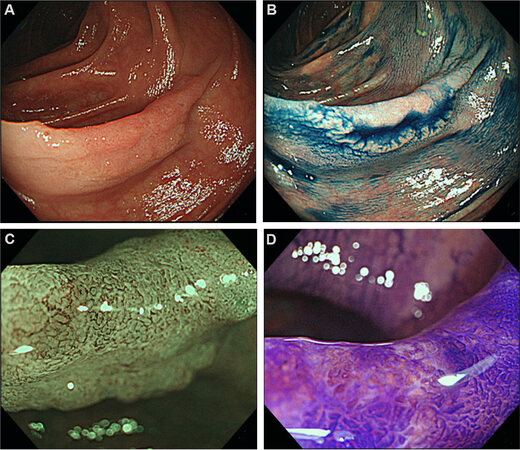
Figure 4. Case presentation: (A, B) 0-IIa (LST-NG) 40 mm in size at transverse colon; (C) magnifying NBI observation revealed JNET 2B; and (D) magnifying endoscopic observation revealed Vi (high grade) pit pattern.
Circumferential incision
First, we injected 0.4% hyaluronic acid with 0.5 mL of indigo carmine and 0.1 mg of epinephrine into the submucosa to elevate the lesion [Figure 5A]. A circumferential incision was initiated from the anal side using the SB Knife Jr [Figure 5B]. One of the blades was placed under the mucosa as if cutting the mucosa with scissors[13]. Then, an incision was made with little tension in the form of a slightly bounced knife. After several incisions for trimming, the scope was slipped under the mucosal layer, and we moved on to the submucosal dissection.
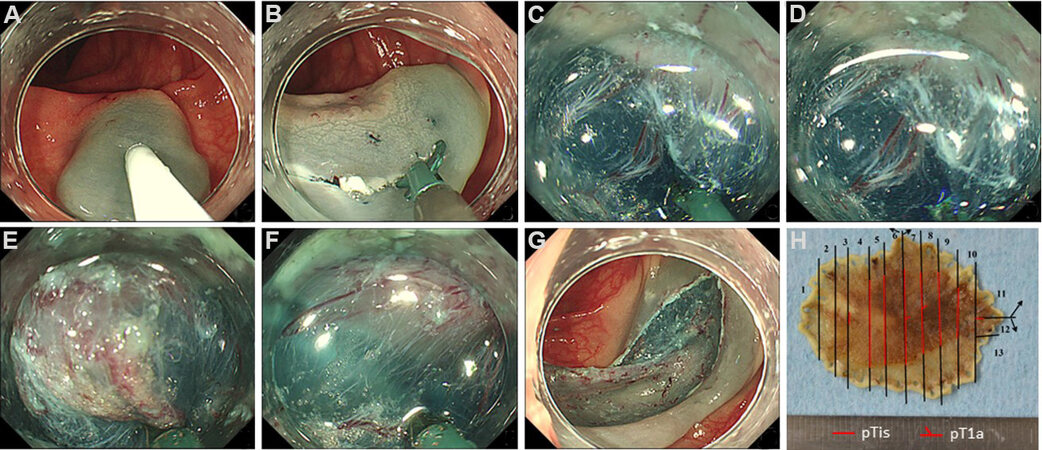
Figure 5. Colorectal endoscopic submucosal dissection (ESD) using the SB Knife Jr: (A) submucosal injection was started from the anal side; (B) circumferential incision similar to cutting paper with scissors; (C) submucosal dissection by grasping the target tissue (1/3 from the bottom of the submucosa); (D) pulling the knife slightly and after confirming the safety and applying the electric current for cutting; (E) prophylactic hemostasis for large vessels; (F) submucosal dissection advanced towards the oral side of the lesion; (G) mucosal defect after en bloc resection; and (H) pathological mapping with the histology showing intramucosal cancer with a negative margin.
Submucosal dissection
The submucosal layer was grasped [Figure 5C], pulled slightly, and a high-frequency electrical current was applied [Figure 5D]. Grasping, pulling, and cutting were performed in a repeated manner. The appropriate depth of submucosal dissection for colorectal ESD using the SB Knife Jr was slightly below the middle portion of the submucosa (1/3 from the bottom of the submucosa). Submucosal dissection was performed with the image of “connecting the dots at the appropriate dissection depth”[13]. Prophylactic hemostasis was performed for large vessels using the SB Knife Jr [Figure 5E].
The incision and dissection were extended towards its right and left sides as needed to maintain a good field of view and adequate depth using the mucosal-flap method. Submucosal dissection was advanced towards the oral side of the lesion, and then the lesion was resected en bloc [Figure 5F and G]. The total procedure time was 57 min. The pathological diagnosis was well-differentiated tubular adenocarcinoma pT1a (SM1/190 μm), 36 mm in diameter. This was a curative resection [Figure 5H].
CONCLUSION
In this article, we focus on the tips and tricks of using the SB Knife Jr for colorectal ESD. The SB Knife Jr has potential advantages, allowing easy and safe colorectal ESD. All the steps of ESD procedures, including mucosal incision, submucosal dissection, and hemostasis, can be achieved with one knife. Complex scope manipulation and advanced endoscopy skill may not be required due to the grasping and cutting technique of this scissor-type knife. Because it is instrumental as a secondary device in difficult situations, we highly recommend that endoscopists master its use.
DECLARATIONS
AcknowledgmentsThe authors extend thanks to Naoko Matsumoto for data collection and administrative assistance.
Authors’ contributionsDesigned the research and wrote the article: Kuwai T
Providing critical intellectual input for the revised manuscript: Tamaru Y, Kusunoki R, Ishaq S
Availability of data and materialsNot applicable.
Financial support and sponsorshipNone.
Conflicts of interestAll authors declared that there are no conflicts of interest.
Ethical approval and consent to participateNot applicable.
Consent for publicationNot applicable.
Copyright© The Authors 2022.
REFERENCES
1. Tanaka S, Kashida H, Saito Y, et al. JGES guidelines for colorectal endoscopic submucosal dissection/endoscopic mucosal resection. Dig Endosc 2015;27:417-34.
2. Tanaka S, Oka S, Chayama K. Colorectal endoscopic submucosal dissection: present status and future perspective, including its differentiation from endoscopic mucosal resection. J Gastroenterol 2008;43:641-51.
3. Hayashi N, Tanaka S, Nishiyama S, et al. Predictors of incomplete resection and perforation associated with endoscopic submucosal dissection for colorectal tumors. Gastrointest Endosc 2014;79:427-35.
4. Tanaka S, Terasaki M, Kanao H, Oka S, Chayama K. Current status and future perspectives of endoscopic submucosal dissection for colorectal tumors. Dig Endosc 2012;24 Suppl 1:73-9.
5. Kuwai T, Yamaguchi T, Imagawa H, et al. Endoscopic submucosal dissection of early colorectal neoplasms with a monopolar scissor-type knife: short- to long-term outcomes. Endoscopy 2017;49:913-8.
6. Honma K, Kobayashi M, Watanabe H, et al. Endoscopic submucosal dissection for colorectal neoplasia. Dig Endosc 2010;22:307-11.
7. Sumida Y, Kuwai T, Ishaq S. Endoscopic submucosal dissection of early gastric neoplasms in the fornix using the newly developed scissor-type SB knife GX. Dig Endosc 2018;30:132.
8. Kuwai T, Yamaguchi T, Imagawa H, et al. Endoscopic submucosal dissection for early esophageal neoplasms using the stag beetle knife. World J Gastroenterol 2018;24:1632-40.
9. Takasago T, Kuwai T, Yamaguchi T, Kohno H, Ishaq S. Endoscopic submucosal dissection with a scissors-type knife for post-EMR recurrence tumor involving the colon diverticulum. VideoGIE 2017;2:211-2.
10. Homma K, Otaki Y, Sugawara M, Kobayashi M. Efficacy of novel SB knife Jr examined in a multicenter study on colorectal endoscopic submucosal dissection. Dig Endosc 2012;24 Suppl 1:117-20.
11. Oka S, Tanaka S, Takata S, Kanao H, Chayama K. Usefulness and safety of SB knife Jr in endoscopic submucosal dissection for colorectal tumors. Dig Endosc 2012;24 Suppl 1:90-5.
12. Tamaru Y, Kuwai T, Ishaq S. Endoscopic submucosal dissection of colorectal tumors using a novel monopolar scissor-type knife “SB Knife Jr.2”. Dig Endosc 2019;31:e105-6.
13. Kuwai T, Tamaru Y, Kuroki K. Tips and fundamentals of colorectal endoscopic submucosal dissection with a scissor-type knife (with videos). Gastroenterological Endoscopy 2019;61:295-308.
14. Yamashina T, Takeuchi Y, Nagai K, et al. Scissor-type knife significantly improves self-completion rate of colorectal endoscopic submucosal dissection: Single-center prospective randomized trial. Dig Endosc 2017;29:322-9.
15. Yoshida N, Dohi O, Inoue K, et al. Efficacy of scissor-type knives for endoscopic mucosal dissection of superficial gastrointestinal neoplasms. Dig Endosc 2020;32:4-15.
16. Akahoshi K, Komori K, Akahoshi K, et al. Advances in endoscopic therapy using grasping-type scissors forceps (with video). World J Gastrointest Surg 2021;13:772-87.
17. Nagai K, Uedo N, Yamashina T, et al. A comparative study of grasping-type scissors forceps and insulated-tip knife for endoscopic submucosal dissection of early gastric cancer: a randomized controlled trial. Endosc Int Open 2016;4:E654-60.
18. Miyakawa A, Kuwai T, Sakuma Y, et al. Learning curve for endoscopic submucosal dissection of early colorectal neoplasms with a monopolar scissor-type knife: use of the cumulative sum method. Scand J Gastroenterol 2020;55:1234-42.
19. Takeuchi Y, Uedo N, Ishihara R, et al. Efficacy of an endo-knife with a water-jet function (Flushknife) for endoscopic submucosal dissection of superficial colorectal neoplasms. Am J Gastroenterol 2010;105:314-22.
Cite This Article
Export citation file: BibTeX | RIS
OAE Style
Kuwai T, Tamaru Y, Kusunoki R, Ishaq S. SB Knife Jr: characteristics and tips on how to use. Mini-invasive Surg 2022;6:16. http://dx.doi.org/10.20517/2574-1225.2021.122
AMA Style
Kuwai T, Tamaru Y, Kusunoki R, Ishaq S. SB Knife Jr: characteristics and tips on how to use. Mini-invasive Surgery. 2022; 6: 16. http://dx.doi.org/10.20517/2574-1225.2021.122
Chicago/Turabian Style
Kuwai, Toshio, Yuzuru Tamaru, Ryusaku Kusunoki, Sauid Ishaq. 2022. "SB Knife Jr: characteristics and tips on how to use" Mini-invasive Surgery. 6: 16. http://dx.doi.org/10.20517/2574-1225.2021.122
ACS Style
Kuwai, T.; Tamaru Y.; Kusunoki R.; Ishaq S. SB Knife Jr: characteristics and tips on how to use. Mini-invasive. Surg. 2022, 6, 16. http://dx.doi.org/10.20517/2574-1225.2021.122
About This Article
Special Issue
Copyright

Data & Comments
Data


 Cite This Article 20 clicks
Cite This Article 20 clicks

 Like This Article 3
likes
Like This Article 3
likes






Comments
Comments must be written in English. Spam, offensive content, impersonation, and private information will not be permitted. If any comment is reported and identified as inappropriate content by OAE staff, the comment will be removed without notice. If you have any queries or need any help, please contact us at support@oaepublish.com.