
Cost-effectiveness of colonoscopy and related procedures: population screening perspectives
 0
0 ,
, Abstract
Colorectal cancer (CRC) screening can reduce the incidence and mortality of CRC, and many countries with moderate-to-high incidences of CRC have implemented population screening programs. Colonoscopy plays a pivotal role in the context of CRC screening as the primary screening modality, the diagnostic exam after a positive noninvasive test, the therapeutic procedure for resecting detected neoplasms, and the surveillance exam after the removal of neoplastic lesions. Although colonoscopy outperforms other noninvasive tests in detecting colorectal neoplasms, it is associated with higher cost, manpower, and invasiveness. Owing to the heterogeneity of healthcare systems in terms of the scale of health revenue, population demographics, and the payment systems in each country, the optimal or most cost-effective screening strategy may vary. Accordingly, economic appraisal of different approaches is essential, especially in organized screening programs within which the resources and the clinical capacity are constrained, and each step of the screening flow needs careful monitoring. The therapeutic procedures applied to manage screening-detected lesions and subsequent surveillance procedures also contribute to substantial additional costs. The level of willingness to pay is affected by various factors, including demographics, income, educational level, and health consciousness, and largely affects the optimal strategies. Herein, we systematically review and summarize the current evidence regarding the cost-effectiveness of colonoscopic screening, related therapeutic procedures, and subsequent surveillance and provide a balanced view from the perspective of population screening programs. It was revealed that 10-year colonoscopy is the most effective strategy compared to other strategies under the higher willingness-to-pay threshold or low colonoscopy cost. There are, however, discrepancies in the results among studies from different countries, which could be associated with the different cost parameters and assumptions used in the models. As for various therapeutic procedures for colorectal neoplasms such as polypectomy, endoscopic mucosal resection, or endoscopic submucosal dissection, strategies based on the risk of advanced histology or deep submucosal invasion based on image-enhanced endoscopy are the least expensive and avoid more recurrences. Furthermore, subsequent surveillance strategies that are based on the risk of CRC are more cost-effective. This article provides a comprehensive review of the literatures and a balanced view from the perspective of population screening programs.
Keywords
INTRODUCTION
Colorectal cancer (CRC) is the second most common cancer in women and the third most common cancer in men worldwide[1]. Early detection of CRC by effective screening strategies and removal of screening-detected adenomatous polyps is the most effective way to reduce the mortality associated with an incidence of CRC[2]. Colonoscopy is the essential process and common pathway of CRC screening and plays a pivotal role in a screening program. Furthermore, patients who have adenomas detected during a colonoscopy are at increased future risk of CRC even after removal of the lesions; therefore, periodic surveillance is indispensable for providing further protection against metachronous CRC[3,4]. The major guidelines currently recommend surveillance intervals based primarily on colonoscopic findings and place special emphasis on the number, size, and histology of detected neoplasms[5-7]. Along with the increasing CRC epidemiology and the launch of population CRC screening in many developed countries, colonoscopy has nowadays become one of the most frequently performed clinical procedures[8]; colonoscopies have become a dominant workload, and the costs of colonoscopies and their related procedures have become a significant financial burden for healthcare systems[9]. The majority of colonic lesions detected by screening, however, are asymptomatic precancerous lesions and early CRCs; thus, subsequent treatment costs could be saved compared with that in the symptomatic clinical stage. Hence, there is a trade-off between the costs of colonoscopies and their related procedures and the treatment of colonic lesions including CRCs. Evolving endoscopic technologies such as endoscopic mucosal resection (EMR) and endoscopic submucosal dissection (ESD) provide less invasive curative treatment options. The appropriate position of ESD in clinical practice is worthy of consideration. In general, ESD is more costly than the traditional polypectomy or EMR, but the expense is much lower than surgery and related expenses (admission fee, anesthesia, etc.). If compared with conventional polypectomy or EMR, it can reduce local recurrence or even post-colonoscopy colorectal cancer (PCCRC); and, if compared with surgery, it can reduce post-treatment morbidity, shorten the duration of admission, and improve the quality of life of the patients. These therapeutic options should be precisely tailored to appropriate lesions that would benefit from individual treatment, thereby balancing effectiveness (PCCRC and CRC mortality), cost, and willingness-to-pay (WTP) levels.
From the population screening perspective, screening logistics involve multiple steps, and each incurs various expenditures. Colonoscopy is the costliest part of the entire screening program, even when considering its related procedures. In this article, we systematically review the current evidence regarding economic appraisals pertaining to colonoscopic screening, therapeutic procedures for screening-detected neoplasms, and subsequent surveillance and provide a balanced view from the perspective of population screening programs.
METHODS
We conducted this systematic review based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines[10] and Cochrane Handbook for systematic reviews[11]. We conducted an electronic search on PubMed and Cochrane databases using the following terms: colonoscopy; colorectal cancer; cost-effectiveness; colorectal cancer screening; surveillance; polypectomy; resect-and-discard; endoscopic mucosal resection; endoscopic submucosal dissection. Our search was restricted to studies written in English and published between January 2012 and December 2021. The titles and abstracts were screened by W.F.H. and H.M.C. to exclude irrelevant studies. The full articles of potentially eligible studies were further reviewed by W.F.H. and H.M.C. independently.
DECISION ANALYSES AND ECONOMIC APPRAISALS OF DIFFERENT CRC SCREENING STRATEGIES: COLONSCOPY VS. VARIOUS NONINVASIVE TESTS
Many previous studies have investigated the economic impact of various CRC screening strategies[12,13]. There are two main CRC screening methods: direct colonoscopy and two-tier noninvasive screening strategies using stool tests, such as guaiac fecal occult blood tests, fecal immunochemical test (FIT), or stool DNA tests, as the primary screening test followed by colonoscopy if positive test results are obtained. Colonoscopy has a higher ability to detect colonic neoplasms, especially early-stage CRC or precancerous neoplasms, than other noninvasive tests but is associated with higher risk and related costs[14]. Moreover, the effectiveness of CRC screening may be offset by the lower participation rate[14]. In addition to colonoscopy, there are several other noninvasive modalities for CRC screening, and these modalities decrease the demand for colonoscopic capacity, hence reducing the incidence of colonoscopy-related complications. Although those modalities may enhance screening participation rate, their ability to detect adenoma and early CRC is inferior to colonoscopy. Eleven studies analyzed the cost-effectiveness of different screening strategies
Overview of cost-effectiveness analyses on different strategies of CRC screening
| Study | Model type | Country | Effectiveness | Adherence rate, % | Screening age, y | Screening strategies | Cost $/per person | LY/QALY | ICER vs. colonoscopy | Optimal strategy at different willingness-to-pay thresholds | ||
| $20,000/LYG | $50,000/LYG | $100,000/LYG | ||||||||||
| Telford | Markov model | Canada | QALY | 73 | 50-75 | 10-year colonoscopy | 1529 | 15.32 | Reference | Colonoscopy | Colonoscopy | Colonoscopy |
| No screening | 783 | 15.20 | 6216.67 | |||||||||
| Annual gFOBT | 1415 | 15.26 | 1900.00 | |||||||||
| Annual FIT | 1437 | 15.30 | 4600.00 | |||||||||
| Knudsen | Microsimulation: MISCAN/SimCRC/CRC-SPIN | US | LY | 100 | 65-80 | 10-year colonoscopy | MISCAN:3840 SimCRC:2680 CRC-SPIN:1980 | MISCAN:0.1516 SimCRC:0.1713 CRC-SPIN:0.1849 | Reference | Colonoscopy | Colonoscopy | Colonoscopy |
| No screening | MISCAN:4030 SimCRC:3540 CRC-SPIN:3000 | MISCAN:0 SimCRC:0 CRC-SPIN:0 | MISCAN: Dominated SimCRC: Dominated CRC-SPIN: Dominated | |||||||||
| Annual FIT | MISCAN:3820 SimCRC:2750 CRC-SPIN:2110 | MISCAN:0.1410 SimCRC:0.1483 CRC-SPIN:0.1504 | MISCAN:1886 SimCRC: Dominated CRC-SPIN: Dominated | |||||||||
| 5-year CTC: DoD | MISCAN:4540 SimCRC:3280 CRC-SPIN:2650 | MISCAN:0.1495 SimCRC:0.1682 CRC-SPIN:0.1777 | MISCAN: Dominated SimCRC: Dominated CRC-SPIN: Dominated | |||||||||
| 5-year CTC: NCTC every 5 years | MISCAN:4590 SimCRC:3350 CRC-SPIN:2700 | MISCAN:0.1427 SimCRC:0.1602 CRC-SPIN:0.1722 | MISCAN: Dominated SimCRC: Dominated CRC-SPIN: Dominated | |||||||||
| Hassan | Markov model | France | LY | 40 | 50-75 | 10-yearly colonoscopy | 1474.73 | 0.04754 | Reference | Biennial FIT | Biennial FIT | Annual FIT |
| No screening | 885.56 | 0 | 12393 | |||||||||
| Annual gFOBT | 995.89 | 0.03994 | 63005 | |||||||||
| Biennial gFOBT | 896.76 | 0.03201 | 37216 | |||||||||
| Annual FIT | 1227.76 | 0.04908 | -160370 | |||||||||
| Biennial FIT | 1026.62 | 0.04538 | 207458 | |||||||||
| 5-year FS | 1117.86 | 0.04517 | 150578 | |||||||||
| 10-year FS | 995.96 | 0.03705 | 45640 | |||||||||
| 5-year CCE | 2022.64 | 0.04901 | 372727 | |||||||||
| 10-year CCE | 1493.90 | 0.04341 | Dominated | |||||||||
| Dan | Markov model | Singapore | QALY | 50 | 50-75 | 10-year colonoscopy | 819 | 16.406* | Reference | Single sigmoidoscopy | FIT | Colonoscopy |
| No screening | 219 | 16.389* | 35294.118 | |||||||||
| Annual FIT | 345 | 16.393* | 36461.538 | |||||||||
| 5-year FS | 426 | 16.394* | 32750 | |||||||||
| 5-year FS +annual FIT | 520 | 16.396* | 29900 | |||||||||
| 5-year Stool DNA | 560 | 16.396* | 25900 | |||||||||
| 5-year CTC | 1086 | 16.406* | Dominated | |||||||||
| Hybrid: FIT+ colonoscopy | 610 | 16.404* | 104500 | |||||||||
| Dinh | Microsimulation | US | QALY | 100 | 50-75 | 10-year colonoscopy | 2082 | 15.79* | Reference | Annual FIT | Annual FIT/Colonoscopy x1 | Concurrent FIT/FS |
| No screening | 3197 | 15.675* | Dominated | |||||||||
| Annual FIT | 1771 | 15.771* | 16368 | |||||||||
| Annual FIT/colonoscopy x1 | 1907 | 15.785* | 35000 | |||||||||
| Concurrent FIT/FS | 1929 | 15.787* | 51000 | |||||||||
| FS | 2118 | 15.746* | Dominated | |||||||||
| Sharaf and Ladabaum | Markov model | US | QALY | 100 | 50-80 | 10-year colonoscopy | 2564 | 18.7443* | - | |||
| No screening | 2364 | 18.6686* | 2642 | |||||||||
| Annual FOBT | 1953 | 18.7352* | 67142 | |||||||||
| Annual FIT | 1866 | 18.7456* | -536923 | |||||||||
| Annual FIT + 5-year FS | 2225 | 18.7469* | -130384 | |||||||||
| 5-yearly FS | 2160 | 18.7372* | 56901 | |||||||||
| Ladabaum | Markov model | Germany | QALY | 100 | 50-75 | 10-year colonoscopy for subjects 55-65 years | 1296.11 | 19.6715* | Reference | FIT | FIT/Colonoscopy 55-65 years | |
| No screening | 2585.4 | 19.5815* | Dominated | |||||||||
| 10-year colonoscopy for subjects 60-70 years | 1350.35 | 19.6524* | Dominated | |||||||||
| FIT※ | 1185.37 | 19.6832* | -9464.96 | |||||||||
| FIT※/colonoscopy 55-65 years | 1240.74 | 19.6872* | -3526.75 | |||||||||
| FIT※/colonoscopy 60-70 years | 1186.5 | 19.6822* | -10243.93 | |||||||||
| Biennial mSEPT9-2well | 2636.29 | 19.6531* | Dominated | |||||||||
| Biennal mSEPT9-3well q2 | 2398.99 | 19.6645* | Dominated | |||||||||
| Annual mSEPT9-2well | 2954.95 | 19.6732* | 975788.24 | |||||||||
| Annual mSEPT9-3well | 2670.19 | 19.6797* | 167570.73 | |||||||||
| Wong | Markov model | Hong Kong | LY, QALY | 60 | 50-75 | 10-year colonoscopy | 4752 | 15.7385/15.3586 | Reference | No-screening | Annual FIT | Annual FIT |
| No screening | 2541 | 15.6420/14.7479 | 22911.92 | |||||||||
| Annual gFOBT | 5349 | 15.7104/15.2339 | Dominated | |||||||||
| Biennial gFOBT | 4221 | 15.6862/15.0687 | 10152.96 | |||||||||
| Annual FIT | 5068 | 15.7650/15.5491 | 11924.53 | |||||||||
| Biennial FIT | 4542 | 15.7429/15.4206 | -47727.27 | |||||||||
| Sekiguchi | Markov model | Japan | QALY | 60 | 40+ | 10-year colonoscopy | 879.384 | 23.1778* | Reference | Colonoscopy | Colonoscopy | Colonoscopy |
| No screening | 1373.9 | 22.7986* | Dominated | |||||||||
| Annual FIT | 833.6504 | 23.0001* | 257.36 | |||||||||
| FIT+ colonoscopy for 50-year-old individuals | 823.0024 | 23.0096* | 335.21 | |||||||||
| Markov model | US | QALY | 100 | 50-80 | 10-year colonoscopy | 4173 | 18.7455* | Reference | Annual FIT | Annual FIT | ||
| No screening | 3020 | 18.6687* | 15013 | |||||||||
| Annual FIT | 2407 | 18.7470* | -1177333 | |||||||||
| Biennial FIT | 2211 | 18.7410* | 436000 | |||||||||
| 3-year MT-sDNA | 5190 | 18.7423* | Dominated | |||||||||
| Barzi | Markov model | US | LY | 46-63 | 50-75 | 10-year colonoscopy | 2861 | 15.227 | Reference | Colonoscopy | Colonoscopy | Colonoscopy |
| Annual gFOBT | 3164 | 15.215 | Dominated | |||||||||
| Biennial gFOBT | 3054 | 15.218 | Dominated | |||||||||
| Annual FIT | 3303 | 15.211 | Dominated | |||||||||
| Biennial FIT | 3186 | 15.215 | Dominated | |||||||||
| 10-year CTC | 3062 | 15.225 | Dominated | |||||||||
| Annual stool DNA | 4296 | 15.216 | Dominated | |||||||||
| Biennial stool DNA | 4161 | 15.219 | Dominated | |||||||||
| Peterse | Microsimulation | US | QALY | 100 | 50-75 | 10-year colonoscopy | 7751 | 0.209 | Reference | Colonoscopy | ||
| No screening | 7286 | 0 | Dominated | |||||||||
| Annual FIT | 6793 | 0.189 | 47900 | |||||||||
| 5-year CTC | 7479 | 0.177 | 8500 | |||||||||
| Biennial mSEPT9 | 8298 | 0.175 | Dominated | |||||||||
| Annual mSEPT9 | 8574 | 0.194 | Dominated | |||||||||
| 10-year PillCam | 8951 | 0.165 | Dominated | |||||||||
| 5-year PillCam | 9940 | 0.196 | Dominated | |||||||||
| 3-yearly MT-sDNA | 8887 | 0.175 | Dominated | |||||||||
| Annual MT-sDNA | 10798 | 0.205 | Dominated | |||||||||
The two-tier screening strategy with the FIT as the primary screening test is currently the most preferred way of providing CRC screening service in regions or countries where endoscopy capacity is constrained. It has nowadays become the mainstay of the stool-based screening approach, as it has the advantage of absolving the need for dietary restriction, has a more user-friendly platform with higher screening participation by the public, and provides higher test performance compared with that of guaiac FOBT[27]. When 10-year colonoscopy was compared with FIT screening strategies (annual/biennial), two studies from the United States reported that colonoscopy screening had an incremental cost-effectiveness ratio (ICER) below $50,000/per quality-adjusted life-year (QALY) and was dominant with 100% certainty[16,25]. Six other studies showed that colonoscopy every 10 years was more costly but with more life-years (LYs)/QALYs gained; hence, it was more cost-effective than the annual FIT screening strategy[15,18,19,23,24.26]. Four studies reported that annual FIT screening was more effective and less costly than 10-year colonoscopy[17,20,21,24]. The results mainly indicate that adherence to the noninvasive screening tests was presumed to be higher than that to the colonoscopy. In two studies, when 10-year colonoscopy was compared with biennial FIT, the former was less cost-effective, and the ICER was higher than $200,000/per LY/QALY[17,24]. One study from Hong Kong reported that biennial FIT was less costly and more effective than colonoscopy every 10 years under the assumption of the same compliance rate of 60% for all screening strategies[22]. Some studies also assessed mixed-method screening with combined FIT and colonoscopy or sigmoidoscopy. In the analysis conducted by Dinh and colleagues, colonoscopy every 10 years was more cost-effective than initial annual FIT/colonoscopy screening once and subsequent annual FIT/sigmoidoscopy screening and had ICERs of $35,000 and $51,000 per QALY gained, respectively[19]. In Ladabaum’s study, hybrid strategies with biennial FIT and colonoscopy had greater effectiveness and lower costs than 10-year colonoscopy[21].
Ladabaum et al.[21] also compared 10-year colonoscopy with blood-based screening using the methylated septin 9 DNA (mSEPT9) test. Compared with colonoscopy every 10 years, annual mSEPT9-based strategies cost more and were less effective with fewer QALYs gained. Biennial mSEPT9-based strategies were cost-effective compared with colonoscopy every ten years, but the ICER was $167,570-975,788 per QALY gained. Multitarget stool DNA (MT-sDNA) every three years was approved by the US Food and Drug Administration (FDA) in 2014[28]. Although the sensitivity of MT-sDNA for CRC was 92.3%, which was much higher than that for FIT, the specificity of MT-sDNA was lower than that of FIT, resulting in an increased demand for colonoscopy and reducing its cost-effectiveness[29]. Another study by Ladabaum et al.[24] showed that, compared with 10-year colonoscopy, 3-year MT-sDNA was more expensive with fewer QALYs gained. In Peterse’s study, compared with colonoscopy every 10 years, mSEPT9 (annual/biennial) and MT-sDNA (annual/3-year) cost more and were less effective with fewer QALYs gained[26].
Virtual colonography with computed tomography colonography (CTC) or MR colonography (MRC) is another noninvasive approach that can potentially be an alternative examination for subjects for whom colonoscopy is not feasible or where colonoscopy capacity or manpower is constrained. Four studies showed that 10-year colonoscopy was more effective and less costly than CTC[16,18,25]. One study showed that 5-year CTC was less cost-effective than 10-year colonoscopy and displayed an ICER of $372,727 per LY gained[17], and another study displayed an ICER of $8500 per QALY gained[26]. Notably, in these five studies, the same compliance rates for CTC and colonoscopy were assumed. Nevertheless, concerns have been raised about CTC because of the potential radiation risks, especially the risk of radiation-related cancer, and the compliance regarding CTC by the public in Asia is rarely reported[30,31]. The compliance rate for CTC may affect screening uptake and overall effectiveness.
Different age groups are associated with different risks of CRC. Precision screening strategies based on different CRC risks are important issues for balancing between effectiveness and usage of relevant resources. Ladabaum et al.[21] compared 10-year colonoscopy, a hybrid strategy with FIT years for ages 50-54 and then colonoscopy starting at age 55 (FIT/COLO 55,65), and a hybrid strategy with FIT years for ages 50-59 and then colonoscopy starting at age 60 (FIT/COLO 60,70). The FIT/COLO 55,65 hybrid strategy was the most effective strategy, followed by FIT and FIT/COLO 60,70 hybrid strategy. At a willingness-to-pay threshold of €50,000 per QALY gained, the FIT/COLO 55,65 hybrid strategy was the optimal strategy. These results reveal that a hybrid strategy with FIT and colonoscopy based on the different CRC risks was a cost-effective approach. Dan et al.[18] reported that a hybrid strategy using FIT for lower-risk patients aged 50-60 years and colonoscopy from ages 60 to 72 years showed it is potentially the most cost-effective strategy. It saves almost as many lives as 10-year colonoscopy but reduces costs by 25% and the number of colonoscopies and screening-related deaths by 35%. These results show that the hybrid strategy with FIT and colonoscopy based on the different risks for CRC was cost-effective. However, there was no relevant cost-effectiveness analysis for the precision screening strategies by the combination of age and other risk factors, and further studies are needed.
The optimal strategies at different WTP levels are shown in Table 1. Two models from the US[16,25] and one model from Canada[15] reported that the optimal strategy was 10-year colonoscopy even at the threshold of $20,000. One model from Japan reported the same results, which may be due to the much lower fee per colonoscopy in Japan than in the US or other countries[23]. Two modeling studies from the US and Singapore reported that the optimal strategy was 10-year colonoscopy at the threshold of $100,000[18,26]. Three models from the US, Hong Kong, and France, however, reported that annual or biennial FIT screening strategies were optimal strategies at the threshold of $50,000[17,22,24].
Therefore, there is no “most recommended” test over the others at this time because the optimal strategy may vary along with the healthcare scenario, medical resources and expenses in individual countries, the WTP threshold of the healthcare payer, and local epidemiology of colorectal neoplasms collectively affect the choice of screening strategies. According to Dan’s study, the cost of colonoscopy and the incidence of CRC were the essential parameters for determining the optimal strategy. When the cost of colonoscopy was less than $300, regardless of the risk of CRC, the strategy of 10-year colonoscopy was the most cost-effective[18]. When the cost of colonoscopy was above $300, FIT was considered the dominant technique at lower incidence levels of CRC. At a higher WTP threshold, the strategy of 10-year colonoscopy was the most effective but required a huge budget and extensive logistic resources.
The quality of colonoscopy also largely impacts the effectiveness of the screening. The adenoma detection rate (ADR), the proportion of subjects with neoplastic lesions detected by colonoscopy among all subjects who undergo colonoscopy, is associated with the risk of incident CRC or CRC death and has been recommended as a key quality benchmark of colonoscopy[32-34]. Hassan et al.[35] reported that colonoscopies performed by endoscopists with low ADRs resulted in a 7% absolute reduction in the CRC incidence prevention rate compared to colonoscopies performed by those with an average ADR (70% vs. 77%). The difference in CRC incidence prevention rate increased to 21% when comparing endoscopists with an average ADR to those with a high ADR. The substantial reduction in the long-term colorectal cancer prevention rate also resulted in substantial losses in LY and economic resources[35].
Cost-effectiveness studies have also compared different scenarios of repeat screening. Greuter et al.[36] reported that virtual colonography as CTC and MRC with more than three screening rounds were cost-effective alternatives for colonoscopy screening. Five rounds of CTC screening were even more effective at lower costs, and the ICER of five rounds of MRC was €3498 per LY gained compared with three rounds of colonoscopy[36]. In Aronsson’s study, repeated colonoscopic screening strategies were more cost-effective than FIT when lifelong effects and costs were considered[37]. Therefore, although a single screening colonoscopy yielded the lowest cost per QALY, 10-year colonoscopy gained additional QALYs at a reasonable cost.
COST-EFFECTIVENESS ANALYSES OF DIFFERENT COLONOSCOPIC TREATMENT STRATEGIES FOR SMALL ADENOMA
A substantial cost of a CRC screening program is represented by endoscopic polypectomy. Furthermore, polypectomy costs are partially related to the cost of pathologic examination. The cost-effectiveness analysis in this regard mainly relates to the “resect-and-discard” strategy[38]. The rationale for the resect-and-discard strategy is based on the low prevalence of advanced histology in small (≤ 1 cm) adenomas, and discarding the specimen without sending it for pathological inspection could substantially reduce the cost. In the colonoscopy-based screening program, Lieberman et al.[39] reported that the proportions of patients in a screening cohort with advanced histology were only 1.7% in the 1-5 mm group and 6.6% in the 6-9 mm group. Gupta et al.[40] also reported that only 0.7% and 0.9% of polyps < 6 mm in size in the right and left colon were advanced neoplasms, respectively.
Image-enhanced endoscopy, such as narrow-band imaging (NBI), outperforms conventional white light colonoscopy in discriminating adenomatous from non-adenomatous colonic polyps with high accuracy[41]. In patients with small polyps (< 10 mm), the application of NBI and the resect-and-discard strategy might correctly guide post-polypectomy surveillance intervals without histopathology information. The American Society for Gastrointestinal Endoscopy (ASGE) developed the Preservation and Incorporation of Valuable Endoscopic Innovations (PIVI) initiative that has set the thresholds for real-time endoscopic assessment of the histology of diminutive colorectal polyps[41]. The threshold in the PIVI document regarding the application of the resect-and-discard strategy for colorectal polyps < 5 mm in size is that endoscopic technology should provide at least 90% agreement in the assignment of the appropriate post-polypectomy surveillance interval. In this context, according to Hassan’s study, the application of the resect-and-discard strategy for diminutive polyps resulted in a savings of $25/person without reducing the screening efficacy. This approach would result in undiscounted annual savings of $33 million for the US population[38]. However, due to the thresholds in the PIVI document being at least 90% in agreement in the assignment of the appropriate post-polypectomy surveillance interval, whether each endoscopy achieves the thresholds with high confidence is still unclear. As Patel et al.[42] reported, previous studies revealed a discrepancy in agreement in surveillance intervals between endoscopists at academic centers and community-based endoscopists. This discrepancy may hinder the applicability of the resect-and-discard strategy and make its cost-effectiveness uncertain. Whether the aforementioned resect-and-discard strategy is similarly applicable to FIT-positive colonoscopy is not clear because the distributions of size and advanced histology of detected adenomas in the FIT-positive population are largely different from the screening colonoscopy cohort (general population of screening age). Hsu et al.[43] analyzed 3920 neoplastic lesions in a FIT-positive colonoscopy cohort and compared them with 9789 neoplastic lesions in a direct screening colonoscopy cohort. Subjects who underwent colonoscopy for positive FIT had a lower prevalence of diminutive polyps (32.2%) than that in the screening colonoscopy cohort (60.5%); therefore, the resect-and-discard strategy in FIT-colonoscopy may not result in a similar degree of cost reduction that observed in the colonoscopy-based screening strategy. Although FIT positivity is associated with an increased likelihood of detecting neoplasms with advanced histology, those diminutive adenomas being detected in FIT-positive subjects were associated with a low risk of advanced histology (4.3%), and none of these patients had invasive cancer; hence, the risk of exposing the patient to undertreatment of invasive cancer by the resect-and-discard strategy is nearly zero. Moreover, compared with histopathological assessment, the agreement in determining surveillance interval by applying the resect-and-discard strategy was as high as 96.5%. Collectively, the resect-and-discard strategy for diminutive polyps in FIT-colonoscopy is feasible and could still save substantial costs making it a cost-effective approach.
COST-EFFECTIVENESS ANALYSIS OF COLONOSCOPIC TREATMENT STRATEGIES FOR LARGE NEOPLASMS
The cost-effectiveness analyses on colonoscopic treatment for large colorectal neoplasms mainly pertain to large flat lesions - laterally spreading tumors (LSTs). The LST was originally proposed by Kudo for tumors that spread extensively and circumferentially along the colonic wall and are larger than 10 mm in diameter[44,45]. EMR is a useful therapeutic technique for LST; however, the maximum diameter of the lesion for en bloc resection is approximately 20 mm, owing to the size of the snare, the technical difficulty, and the perforation risk[46]. For LSTs larger than 20 mm, the piecemeal EMR (pEMR) technique is commonly used, but it may be associated with a higher risk of recurrence[47-49]. In Yamada’s study, LSTs with the presence of a large nodule, a depression, and an invasive pit pattern under magnified chromoendoscopy had a higher risk of deep submucosal invasion[50]. Due to the substantial risk of submucosal invasion and multifocal invasion, en bloc resection with ESD techniques could be reserved for some specific lesions as an alternative procedure to more invasive surgery[51]. Universal treatment with ESD for all LSTs larger than 20 mm may not be cost-effective because of its technical difficulty with a long procedure time, higher cost for the devices, and higher risk of perforation complications. In Bahin’s study, the cost-effectiveness of three strategies for removing large LSTs > 20 mm was compared: (1) wide-field endoscopic mucosal resection (WF-EMR); (2) universal endoscopic submucosal dissection (U-ESD); and (3) selective ESD (S-ESD)[52]. In the WF-EMR strategy, lesions classified as highly suspicious for submucosal invasive cancer (SMIC) were referred for surgical management, suspicious rectal lesions classified as low-risk SMIC were referred for transanal excision, and all other lesions were treated via WF-EMR. In the U-ESD strategy, all lesions were initially treated by ESD regardless of SMIC suspicion. In the S-ESD strategy, lesions with high suspicion for SMIC were treated with ESD; others were treated with WF-EMR. S-ESD was the least expensive strategy and more effective than WF-EMR by preventing 19 additional surgeries per 1000 patients. Compared with S-ESD, U-ESD prevented another 13 surgeries at an incremental cost per surgery of $210,112[52]. Therefore, S-ESD is the preferred treatment strategy for large LSTs [Table 2].
Overview of the cost-effectiveness analyses of the different endoscopic treatment strategies for LST
| Study | Country | Effectiveness measurement | Patients | Treatment strategies | Cost ($) | Effectiveness | ICER |
| Bahin | Australia | Number of surgeries avoided | laterally spreading colorectal lesions (LSLs) > 20 mm | Selective ESD | 4224 per 1000 cases | 925 surgeries avoided | Reference |
| WF-EMR | 4335 per 1000 cases | 906 surgeries avoided | Dominated | ||||
| Universal ESD | 6912 | 938 surgeries avoided | 210112 | ||||
| Sekiguchi | Japan | An avoid recurrence/an avoid surgery | Colonic LST-NG ≥ 2 cm | pEMR | 1948 | - | Reference |
| ESD | 2834 | NNB by preventing a recurrence: 4/NNB by preventing a surgery: 78.7 | 3575/69604 | ||||
| Rectal LST-NG ≥ 2 cm | pEMR | 3555 | - | Reference | |||
| ESD | 4469 | NNB by preventing a recurrence: 4.9/NNB by preventing a surgery: 84.7 | 4521/77689 | ||||
| Colonic LST-G-M ≥ 3 cm | pEMR | 2042 | - | Reference | |||
| ESD | 2969 | NNB by preventing a recurrence: 4.2/NNB by preventing a surgery: 82 | 3883/76118 | ||||
| Rectal LST-G-M ≥ 3 cm | pEMR | 2903 | - | Reference | |||
| ESD | 3812 | NNB by preventing a recurrence: 4.2/NNB by preventing a surgery: 82 | 4146/70505 | ||||
| Swedish | An avoid recurrence/an avoid surgery | Colonic LST-NG ≥ 2 cm | pEMR | 5335 | - | Reference | |
| ESD | 3438 | - | Dominant | ||||
| Rectal LST-NG ≥ 2 cm | pEMR | 9682 | - | Reference | |||
| ESD | 8609 | - | Dominant | ||||
| Colonic LST-G-M ≥ 3 cm | pEMR | 5495 | - | Reference | |||
| ESD | 3780 | - | Dominant | ||||
| Rectal LST-G-M ≥ 3 cm | pEMR | 7890 | - | Reference | |||
| ESD | 6878 | - | Dominant |
LSTs are macroscopically classified into granular (LST-G) and nongranular types (LST-NG). LST-G is further subclassified into homogeneous (LST-G-H) and nodular mixed (LST-G-M) types. LST-NG is further subclassified into flat elevated (LST-NG-F) and pseudo-depressed (LST-NG-PD) types. Such a classification is clinicopathologically relevant, and one meta-analysis showed that LST-NG-PD had an extraordinarily higher risk of SMIC (31.6%) than LST-NG-FE (4.9%), LST-G-H (0.5%), and LST-G-NM (10.5%), and SMIC was more common in distally located LSTs than in proximally located LSTs (odds ratio: 2.50; 95%CI: 1.24-5.02)[53]. Sekiguchi et al.[54] reported that, for colon/rectal LST-NG ≥ 2 cm and LST-G-M ≥ 3 cm, when compared with pEMR, ESD was more cost-effective with a higher cost that was offset by fewer recurrences and surgeries. The ICERs for avoided recurrence and surgery for ESD against pEMR were $3575-4521 and $69,604-77,689, respectively. The probability of ESD being chosen as a more cost-effective option than pEMR was > 50% at willingness-to-pay values of ≥ $3795-4744 for avoiding recurrence and ≥ $90,143-99,631 for avoiding surgery[53]. Due to the higher cost of ESD, whether the ESD strategy is cost-effective depends not only on cost settings but also on the skill level of the endoscopist, which largely affects the time cost of ESD as well as the WTP value for avoiding recurrence/surgery. Further study is warranted.
COST-EFFECTIVENESS ANALYSES OF DIFFERENT COLONOSCOPIC SURVEILLANCE STRATEGIES
Determination of the surveillance interval after colonoscopy is currently based on the risk level as determined by colonoscopic findings[5]. Sonnenberg’s study reported that the most common reason for performing colonoscopy is surveillance of previously discovered colorectal neoplasia, either adenoma or cancer[8]. Five studies assessed the cost-effectiveness of colonoscopic surveillance strategies with different surveillance intervals in patients with adenomas [Table 3][55-59]. Four studies reported that, compared with no surveillance strategy, colonoscopic surveillance strategies were more costly but had more LY/QALY gain, making them more cost-effective strategies[55-58]. Only one study showed that colonoscopic surveillance strategies were less costly with more QALY gain[59]. In Arguedas’ study, colonoscopic surveillance every three years for patients with large adenoma and five years for patients with small adenoma or without adenoma were cost-effective and had an ICER of $27,970 per LY gained compared to no surveillance[55]. Shaukat et al.[56] also reported that colonoscopy surveillance every three years for patients with large adenoma and every five years for patients with small adenoma or without adenoma was cost-effective and had an ICER of $20,600 per LY gained. Saini et al.[58] found that, compared with no surveillance (colonoscopy every 10 years for patients with any endoscopic finding), the strategy of colonoscopy surveillance every 3 years for high-risk patients and 10 years for low-risk patients was highly cost-effective, with an ICER of $5743 per QALY gained. In contrast, the strategy of colonoscopic surveillance every three years for high-risk patients and five years for low-risk patients was relatively expensive, with an ICER of $296,266 per QALY gain. The strategy of colonoscopy surveillance every three years for all patients only resulted in additional cost and harm. Hassan et al.[57] simulated 60-year-old patients with adenoma and found that single colonoscopy surveillance after one year was cost-effective, with an ICER of $66,136 per LY gained. These results reveal the relatively high prevalence of CRC one year after clearing polypectomy and a relative deficiency of the current guidelines to exclude a clinically meaningful risk of CRC after polypectomy[57]. Meester et al.[59] conducted a cost-effectiveness analysis of different screening strategies. In patients with low-risk adenomas in the FIT screening program, the risk of CRC incidence and mortality was higher than those with LRAs in the colonoscopy screening program. Thus, the cost-effectiveness ratio for high-intensity surveillance (5 years) versus low-intensity surveillance (10 years) was more favorable (ICER = $11,100 per QALY gained) than in patients with low-risk adenomas in the colonoscopy screening program. However, the overall risk and benefit of surveillance in patients with high-risk adenomas in the FIT screening program versus in the colonoscopy screening program were similar. The ICERs for high-intensity surveillance (three years) versus low-intensity surveillance for patients with high-risk adenomas were similar ($11,100 per QALY gained) in the FIT and colonoscopy screening programs[59].
Overview of the cost-effectiveness analyses on different colonoscopic surveillance strategies
| Study | Model type | Country | Effectiveness | Participants | Screening strategy | Surveillance strategy | Cost per person | LY/QALY | ICER |
| Arguedas | Markov model | US | LY | 50-year-old patients with adenomas | No surveillance | 1014 | 8.45 | Reference | |
| Colonoscopy 3 years than 5 years | 1572 | 8.48 | 27970 | ||||||
| Celecoxib | 11503 | 8.49 | 1715199 | ||||||
| Shaukat | Markov model | US | LY | 50-year-old patients with adenomas | No surveillance | 2796 | 18.64 | Reference | |
| Colonoscopy 3 years for large adenoma, 5 years for small or no adenoma | 4579 | 18.72 | 20600 | ||||||
| Hassan | Simple decision tree | Italy | LY | 60-year-old patients with adenomas | No surveillance | - | - | Reference | |
| Colonoscopy after 1 year | - | - | 66136 | ||||||
| Saini | Markov model | US | QALY | 50-year-old patients with adenomas | No surveillance | 1775 | 17.57 | Reference | |
| Colonoscopy 3 years for HR, 10 years for LR | 1831 | 17.58 | 5734 | ||||||
| Colonoscopy 3 years for HR, 5 years for LR | 3170 | 17.58 | 296266 | ||||||
| Colonoscopy 3 years for HR, and LR | 4936 | 17.58 | 316100 | ||||||
| Meester | Microsimulation | US | QALY | 50-year-old patients with LRA | Colonoscopy | No Surveillance | 4110 | 19.456 | Dominated |
| Colonoscopy after 10 years | 3870 | 19.570 | Reference | ||||||
| Colonoscopy 10 years for LR, 5 years for HR | 3898 | 19.577 | 4000 | ||||||
| Colonoscopy 5 years for LR, 3 years for HR | 4290 | 19.589 | 18400 | ||||||
| FIT | No Surveillance | 4699 | 19.407 | Dominated | |||||
| Colonoscopy after 10 years | 4536 | 19.510 | Dominated | ||||||
| Colonoscopy 10 years for LR, 5 years for HR | 4454 | 19.530 | Reference | ||||||
| Colonoscopy 5 years for LR, 3 years for HR | 4841 | 19.565 | 11100 | ||||||
| 50-year-old patients with HRA | Colonoscopy | No Surveillance | 6622 | 19.303 | Dominated | ||||
| Colonoscopy after 10 years | 5633 | 19.491 | Reference | ||||||
| Colonoscopy 10 years for LR, 5 years for HR | 5784 | 19.525 | 4500 | ||||||
| Colonoscopy 5 years for LR, 3 years for HR | 6052 | 19.557 | 8400 | ||||||
| FIT | No Surveillance | 6608 | 19.302 | Dominated | |||||
| Colonoscopy after 10 years | 6113 | 19.462 | Dominated | ||||||
| Colonoscopy 10 years for LR, 5 years for HR | 5856 | 19.520 | Reference | ||||||
| Colonoscopy 5 years for LR, 3 years for HR | 6131 | 19.553 | 8400 |
Recent studies have shown the usefulness of using FIT in detecting advanced neoplasms during colonoscopic surveillance intervals. For example, Cross et al.[60] reported that in intermediate-risk patients (with three to four adenomas < 10 mm or at least one ≥ 10 mm), the cumulative sensitivity and specificity for CRC of three rounds of annual FIT with low threshold levels for fecal hemoglobin (10 µg/g) were 91.7% (95 %CI: 73.0 - 99.0) and 69.8 % (95 %CI: 68.5 - 71.1), respectively. However, in this study, the three-year program sensitivities for CRC and advanced adenomas of annual FIT at the threshold level of 10 µg/g were 72% and 57%, respectively. This strategy would result in 28% of CRCs and 43% of advanced adenomas being missed compared with three-year colonoscopic surveillance[60]. A recent study by Peng et al.[61] from the Taiwan CRC Screening Program revealed that those who received subsequent FIT after negative colonoscopy had a significantly lower risk of incident CRCs than those who did not, which was assumed to be mainly attributable to the detection of noncancerous advanced adenoma that might have been missed at the initial colonoscopy. Whether such an “interval-FIT” approach could become a cost-effective alternative or an adjunctive approach to colonoscopic surveillance is largely unknown and requires further study.
EMERGING ISSUES THAT REQUIRE FURTHER EXPLORATION
Although colonoscopy and related procedures are cost-effective for CRC screening and post-polypectomy surveillance, there are still some issues that require further exploration [Table 4]. First, the application of new technologies such as artificial intelligence (AI) in colonoscopy is now attracting substantial attention, and its cost-effectiveness is worthy of investigation[62]. The major roles of CAD during colonoscopy include computer-aided detection (CADe) and computer-aided characterization (CADx)[63]. CADe helps endoscopists detect polyps that could be overlooked visually, and CADx improves accurate characterization by optical biopsy[63]. Mori et al.[64] demonstrated that the use of AI enabled the “diagnose-and-leave” strategy and resulted in substantial cost reductions for colonoscopy compared with the resect-all-polyps strategy. However, there remains no comprehensive cost-effectiveness analysis conducted for the application of AI in colonoscopy. This is because this technology is still in its primitive stage, and many clinical and cost parameters remain unclear. For example, AI tools can increase the detection of small adenoma, and it may result in a substantial increment in the pathologic examination cost. Moreover, it remains unclear for which level of endoscopists AI is most beneficial; therefore, using universal ADR parameters may lead to an erroneous conclusion. Further study is anticipated. Second, exploration of the cost-effectiveness of CRC screening with different strategies in young (40-49 years) adults is an emerging issue due to the increasing incidence of young-onset CRC in many countries[65,66]. According to the recent modeling study by the US Preventive Services Task Force, if screening were to begin at age 45 years instead of age 50, the models of CRC screening strategies with stool tests, colonoscopy, or CTC showed 22-27 additional LY gained (8%-9% increase) and required 161-784 additional colonoscopies (10%-23% increase) per 1000 persons, and these results suggest that CRC screening starting at age 45 years provides an efficient balance of colonoscopy burden and life-years gained[67]. Given the different young-onset CRC epidemiology and the healthcare facts across different countries, further cost-effectiveness analysis studies based on local scenarios are needed. Third, omics technology has provided integrated proteogenomic analysis for precision medicine, especially for cancer prevention. Targeted population screening for CRC would reduce the burden and demand for colonoscopy[68]. Comprehensive assessment of the risk of CRC and the development of reliable and verifiable risk stratification tools that can be used in the clinic are essential. Three studies reported that the current uniform colonoscopy screening strategy appeared more cost-effective than personalized risk-based screening strategies based on polygenic risk profile and family history[69-71]. However, cost-effectiveness is highly dependent on the costs of determining risk, and such costs may decrease in the future along with the further advance of omic technologies. Furthermore, cost-effectiveness analysis studies for personalized CRC screening with different strategies are needed. Fourth, endoscopic full-thickness resection (EFTR) has been demonstrated to be effective and safe for non-lifting and difficult lesions[72]. Only one cost-effectiveness analysis study reported that the mean costs per R0 resection were €3708.98 for EFTR, €3115.10 for standard endoscopic resection, and €8924.05 for surgical treatment. EFTR is cost-effective in comparison with surgical and endoscopic treatment for colonic non-lifting and difficult lesions[73]. Moreover, long-term follow-up is also needed to further assess the cost-effectiveness of EFTR. Fifth, many assumptions in the cost-effectiveness analyses limit the validity of those studies. For example, colonoscopy quality or skill level of endoscopic diagnosis (ability to accurately diagnose neoplasms and estimate invasion depth) or treatment such as polypectomy/EMR/ESD by individual endoscopists were assumed to be consistent in most of the cost-effectiveness models. Furthermore, the payment for colonoscopy varies greatly from country to country and ranges from $45.2 to $1695. Colonoscopy payments tend to be higher in countries with higher gross domestic products (GDPs) per capita, but a significant discrepancy still exists even within the same category of GDP level [Figure 1 and Supplementary Table 1], which has a significant impact on the results of cost-effectiveness analyses and the optimal strategies. When the payment for colonoscopy is low, colonoscopy-based screening or more frequent surveillance strategies will become the dominant or more cost-effective strategy over other noninvasive or less intensive strategies. More comprehensive cost-effectiveness analysis studies that take into account the diversity of neoplasms, heterogeneity of the clinical practice scenario, or the existing comorbidities of the patients are needed.
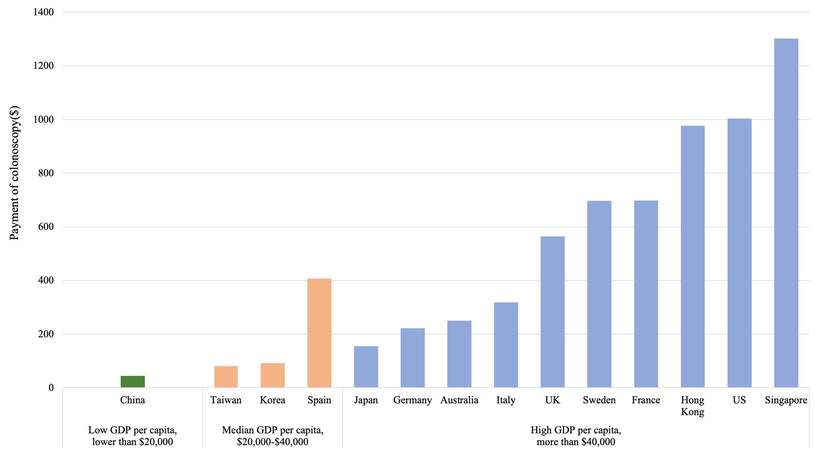
Figure 1. Payment of colonoscopy worldwide in 2020.
Emerging cost-effectiveness issues that are worthwhile to investigate
| Potential cost-effectiveness issues |
| • Application of AI in colonoscopy: CADe and CADx • EFTR for difficult colonic lesions • ESD vs. pEMR for large colorectal neoplasms (i.e., LST) at different endoscopist skill levels and payment levels • CRC screening with different strategies for young (40-49 years) adults • Endoscopic vs. surgery for superficial T1 CRC • Noninvasive tests (FIT, MT-sDNA, etc.) vs. colonoscopy as the surveillance tool • Noninvasive tests (FIT, MT-sDNA, etc.) vs. colonoscopy as the screening tool for subjects with a family history of CRC |
CONCLUSIONS
Gaps between limited healthcare resources and expanding healthcare service demands, and the development of new technologies have become a significant pressure on many healthcare systems worldwide and generate the demand for comprehensive health technology assessment, including economic appraisals, for scientific policymaking. Our current review provides updates on the economic appraisal of colonoscopic practices and their related procedures in the context of population CRC screening and surveillance. Many of the cost-effective strategies have been implemented in our current practice, but some have not, which may be due to the insufficient diversity being accommodated in the parameters or assumptions used in the analyses and the limited number of high-quality studies or clinical trials from which parameters were derived. Finally, whether a cost-effective strategy is applicable to the individual program still needs careful and specific consideration, which must include the healthcare context and the availability of certain services in the individual countries or healthcare systems, patient preference, and WTP levels.
DECLARATIONS
Authors’ contributionsConcept and design of the article: Chiu HM
Literature review: Hsu WF
Drafting of the manuscript: Hsu WF, Chiu HM
Availability of data and materialsNot applicable.
Financial support and sponsorshipThis study was partially supported by the Health Promotion Administration, Ministry of Health and Welfare. (A1091116).
Conflicts of interestBoth authors have no conflict of interest to be declared regarding this manuscript.
Ethical approval and consent to participateNot applicable.
Consent for publicationNot applicable.
Copyright© The Author(s) 2022.
Supplementary MaterialsREFERENCES
1. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: globocan estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2021;71:209-49.
2. Chiu HM, Jen GH, Wang YW, et al. Long-term effectiveness of faecal immunochemical test screening for proximal and distal colorectal cancers. Gut 2021;70:2321-9.
3. Winawer SJ, Zauber AG, Ho MN, et al. Prevention of Colorectal Cancer by Colonoscopic Polypectomy. N Engl J Med 1993;329:1977-81.
4. Zauber AG, Winawer SJ, O’Brien MJ, et al. Colonoscopic polypectomy and long-term prevention of colorectal-cancer deaths. N Engl J Med 2012;366:687-96.
5. Gupta S, Lieberman D, Anderson JC, et al. Recommendations for follow-up after colonoscopy and polypectomy: a consensus update by the us multi-society task force on colorectal cancer. Gastrointest Endosc 2020;91:463-485.e5.
6. Rutter MD, East J, Rees CJ, et al. British society of gastroenterology/association of coloproctology of great Britain and Ireland/public health England post-polypectomy and post-colorectal cancer resection surveillance guidelines. Gut 2020;69:201-23.
7. Hassan C, Antonelli G, Dumonceau JM, et al. Post-polypectomy colonoscopy surveillance: european society of gastrointestinal endoscopy (ESGE) guideline - update 2020. Endoscopy 2020;52:687-700.
8. Sonnenberg A, Amorosi SL, Lacey MJ, Lieberman DA. Patterns of endoscopy in the United States: analysis of data from the centers for medicare and medicaid services and the national endoscopic database. Gastrointest Endosc 2008;67:489-96.
9. Harewood G. Colonoscopy practice patterns since introduction of medicare coverage for average-risk screening. Clinical Gastroenterology and Hepatology 2004;2:72-7.
10. Moher D, Shamseer L, Clarke M, et al. PRISMA-P Group. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst Rev 2015;4:1.
11. Higgins J, Thomas J. Cochrane handbook for systematic reviews of interventions. Available from: https://training.cochrane.org/handbook/current [Last accessed on 20 Apr 2022].
12. Pignone M, Saha S, Hoerger T, Mandelblatt J. Cost-effectiveness analyses of colorectal cancer screening: a systematic review for the U.S. preventive services task force. Ann Intern Med 2002;137:96-104.
13. Lansdorp-Vogelaar I, Knudsen AB, Brenner H. Cost-effectiveness of colorectal cancer screening. Epidemiol Rev 2011;33:88-100.
14. Quintero E, Castells A, Bujanda L, et al. COLONPREV Study Investigators. Colonoscopy versus fecal immunochemical testing in colorectal-cancer screening. N Engl J Med 2012;366:697-706.
15. Telford JJ, Levy AR, Sambrook JC, Zou D, Enns RA. The cost-effectiveness of screening for colorectal cancer. CMAJ 2010;182:1307-13.
16. Knudsen AB, Lansdorp-Vogelaar I, Rutter CM, et al. Cost-effectiveness of computed tomographic colonography screening for colorectal cancer in the medicare population. J Natl Cancer Inst 2010;102:1238-52.
17. Hassan C, Benamouzig R, Spada C, et al. Cost effectiveness and projected national impact of colorectal cancer screening in France. Endoscopy 2011;43:780-93.
18. Dan YY, Chuah BY, Koh DC, Yeoh KG. Screening based on risk for colorectal cancer is the most cost-effective approach. Clin Gastroenterol Hepatol 2012;10:266-71.e1.
19. Dinh T, Ladabaum U, Alperin P, Caldwell C, Smith R, Levin TR. Health benefits and cost-effectiveness of a hybrid screening strategy for colorectal cancer. Clin Gastroenterol Hepatol 2013;11:1158-66.
20. Sharaf RN, Ladabaum U. Comparative effectiveness and cost-effectiveness of screening colonoscopy vs. sigmoidoscopy and alternative strategies. Am J Gastroenterol 2013;108:120-32.
21. Ladabaum U, Alvarez-Osorio L, Rösch T, Brueggenjuergen B. Cost-effectiveness of colorectal cancer screening in Germany: current endoscopic and fecal testing strategies versus plasma methylated Septin 9 DNA. Endosc Int Open 2014;2:E96-E104.
22. Wong CK, Lam CL, Wan YF, Fong DY. Cost-effectiveness simulation and analysis of colorectal cancer screening in Hong Kong Chinese population: comparison amongst colonoscopy, guaiac and immunologic fecal occult blood testing. BMC Cancer 2015;15:705.
23. Sekiguchi M, Igarashi A, Matsuda T, et al. Optimal use of colonoscopy and fecal immunochemical test for population-based colorectal cancer screening: a cost-effectiveness analysis using Japanese data. Jpn J Clin Oncol 2016;46:116-25.
24. Ladabaum U, Mannalithara A. Comparative effectiveness and cost effectiveness of a multitarget stool DNA test to screen for colorectal neoplasia. Gastroenterology 2016;151:427-439.e6.
25. Barzi A, Lenz HJ, Quinn DI, Sadeghi S. Comparative effectiveness of screening strategies for colorectal cancer. Cancer 2017;123:1516-27.
26. Peterse EFP, Meester RGS, de Jonge L, et al. Comparing the cost-effectiveness of innovative colorectal cancer screening tests. J Natl Cancer Inst 2021;113:154-61.
27. Smith A, Young GP, Cole SR, Bampton P. Comparison of a brush-sampling fecal immunochemical test for hemoglobin with a sensitive guaiac-based fecal occult blood test in detection of colorectal neoplasia. Cancer 2006;107:2152-9.
28. Jaklevic MC. Pandemic spotlights in-home colon cancer screening tests. JAMA 2020; doi: 10.1001/jama.2020.22466.
29. Imperiale TF, Ransohoff DF, Itzkowitz SH, et al. Multitarget stool DNA testing for colorectal-cancer screening. N Engl J Med 2014;370:1287-97.
30. Neri E, Faggioni L, Cerri F, et al. CT colonography versus double-contrast barium enema for screening of colorectal cancer: comparison of radiation burden. Abdom Imaging 2010;35:596-601.
31. Hirofuji Y, Aoyama T, Koyama S, Kawaura C, Fujii K. Evaluation of patient dose for barium enemas and CT colonography in Japan. Br J Radiol 2009;82:219-27.
32. Rex DK, Schoenfeld PS, Cohen J, et al. Quality indicators for colonoscopy. Gastrointest Endosc 2015;81:31-53.
33. Kaminski MF, Regula J, Kraszewska E, et al. Quality indicators for colonoscopy and the risk of interval cancer. N Engl J Med 2010;362:1795-803.
34. Corley DA, Jensen CD, Marks AR, et al. Adenoma detection rate and risk of colorectal cancer and death. N Engl J Med 2014;370:1298-306.
35. Hassan C, Rex DK, Zullo A, Kaminski MF. Efficacy and cost-effectiveness of screening colonoscopy according to the adenoma detection rate. United European Gastroenterol J 2015;3:200-7.
36. Greuter MJ, Berkhof J, Fijneman RJ, et al. The potential of imaging techniques as a screening tool for colorectal cancer: a cost-effectiveness analysis. Br J Radiol 2016;89:20150910.
37. Aronsson M, Carlsson P, Levin LÅ, Hager J, Hultcrantz R. Cost-effectiveness of high-sensitivity faecal immunochemical test and colonoscopy screening for colorectal cancer. Br J Surg 2017;104:1078-86.
38. Hassan C, Pickhardt PJ, Rex DK. A resect and discard strategy would improve cost-effectiveness of colorectal cancer screening. Clin Gastroenterol Hepatol 2010;8:865-9, 869.e1.
39. Lieberman D, Moravec M, Holub J, Michaels L, Eisen G. Polyp size and advanced histology in patients undergoing colonoscopy screening: implications for CT colonography. Gastroenterology 2008;135:1100-5.
40. Gupta N, Bansal A, Rao D, et al. Prevalence of advanced histological features in diminutive and small colon polyps. Gastrointest Endosc 2012;75:1022-30.
41. Dayyeh BK, Thosani N, Konda V, et al; ASGE Technology Committee. ASGE technology committee systematic review and meta-analysis assessing the ASGE PIVI thresholds for adopting real-time endoscopic assessment of the histology of diminutive colorectal polyps. Gastrointest Endosc 2015;81:502.e1-502.e16.
42. Patel SG, Schoenfeld P, Kim HM, et al. Real-time characterization of diminutive colorectal polyp histology using narrow-band imaging: implications for the resect and discard strategy. Gastroenterology 2016;150:406-18.
43. Hsu WF, Cheng SY, Shun CT, et al. Higher risk of advanced histology in adenoma less than 10 mm in fecal immunochemical test screening: Implication for management. J Gastroenterol Hepatol 2020;35:1738-45.
44. Kudo S. Endoscopic mucosal resection of flat and depressed types of early colorectal cancer. Endoscopy 1993;25:455-61.
45. Kudo SE, Takemura O, Ohtsuka K. Flat and depressed types of early colorectal cancers: from East to West. Gastrointest Endosc Clin N Am 2008;18:581-93, xi.
46. Tanaka S, Oka S, Kaneko I, et al. Endoscopic submucosal dissection for colorectal neoplasia: possibility of standardization. Gastrointest Endosc 2007;66:100-7.
47. Brooker JC, Saunders BP, Shah SG, Thapar CJ, Suzuki N, Williams CB. Treatment with argon plasma coagulation reduces recurrence after piecemeal resection of large sessile colonic polyps: a randomized trial and recommendations. Gastrointest Endosc 2002;55:371-5.
48. Conio M, Repici A, Demarquay J, Blanchi S, Dumas R, Filiberti R. EMR of large sessile colorectal polyps. Gastrointestinal Endoscopy 2004;60:234-41.
49. Horiki N, Omata F, Uemura M, et al. Risk for local recurrence of early gastric cancer treated with piecemeal endoscopic mucosal resection during a 10-year follow-up period. Surg Endosc 2012;26:72-8.
50. Yamada M, Saito Y, Sakamoto T, et al. Endoscopic predictors of deep submucosal invasion in colorectal laterally spreading tumors. Endoscopy 2016;48:456-64.
51. Gotoda T, Kondo H, Ono H, et al. A new endoscopic mucosal resection procedure using an insulation-tipped electrosurgical knife for rectal flat lesions: report of two cases. Gastrointestinal Endoscopy 1999;50:560-3.
52. Bahin FF, Heitman SJ, Rasouli KN, et al. Wide-field endoscopic mucosal resection versus endoscopic submucosal dissection for laterally spreading colorectal lesions: a cost-effectiveness analysis. Gut 2018;67:1965-73.
53. Bogie RMM, Veldman MHJ, Snijders LARS, et al. Endoscopic subtypes of colorectal laterally spreading tumors (LSTs) and the risk of submucosal invasion: a meta-analysis. Endoscopy 2018;50:263-82.
54. Sekiguchi M, Igarashi A, Mizuguchi Y, et al. Cost-effectiveness analysis of endoscopic resection for colorectal laterally spreading tumors: Endoscopic submucosal dissection versus piecemeal endoscopic mucosal resection. Dig Endosc 2022;34:553-68.
55. Arguedas MR, Heudebert GR, Wilcox CM. Surveillance colonoscopy or chemoprevention with COX-2 inhibitors in average-risk post-polypectomy patients: a decision analysis. Aliment Pharmacol Ther 2001;15:631-8.
56. Shaukat A, Parekh M, Lipscomb J, Ladabaum U. Can calcium chemoprevention of adenoma recurrence substitute or serve as an adjunct for colonoscopic surveillance? Int J Technol Assess Health Care 2009;25:222-31.
57. Hassan C, Pickhardt PJ, Di Giulio E, Kim DH, Zullo A, Morini S. Cost-effectiveness of early one-year colonoscopy surveillance after polypectomy. Dis Colon Rectum 2009;52:964-71; discussion 971.
58. Saini SD, Schoenfeld P, Vijan S. Surveillance colonoscopy is cost-effective for patients with adenomas who are at high risk of colorectal cancer. Gastroenterology 2010;138:2292-9, 2299.e1.
59. Meester RGS, Lansdorp-Vogelaar I, Winawer SJ, Zauber AG, Knudsen AB, Ladabaum U. High-intensity versus low-intensity surveillance for patients with colorectal adenomas: a cost-effectiveness analysis. Ann Intern Med 2019;171:612-22.
60. Cross AJ, Wooldrage K, Robbins EC, et al. Faecal immunochemical tests (FIT) versus colonoscopy for surveillance after screening and polypectomy: a diagnostic accuracy and cost-effectiveness study. Gut 2019;68:1642-52.
61. Peng SM, Hsu WF, Wang YW, et al. Faecal immunochemical test after negative colonoscopy may reduce the risk of incident colorectal cancer in a population-based screening programme. Gut 2021;70:1318-24.
62. Liedlgruber M, Uhl A. Computer-aided decision support systems for endoscopy in the gastrointestinal tract: a review. IEEE Rev Biomed Eng 2011;4:73-88.
63. Misawa M, Kudo SE, Mori Y, et al. Current status and future perspective on artificial intelligence for lower endoscopy. Dig Endosc 2021;33:273-84.
64. Mori Y, Kudo SE, East JE, et al. Cost savings in colonoscopy with artificial intelligence-aided polyp diagnosis: an add-on analysis of a clinical trial (with video). Gastrointest Endosc 2020;92:905-911.e1.
65. Vuik FE, Nieuwenburg SA, Bardou M, et al. Increasing incidence of colorectal cancer in young adults in Europe over the last 25 years. Gut 2019;68:1820-6.
66. Howren A, Sayre EC, Loree JM, et al. Trends in the incidence of young-onset colorectal cancer with a focus on years approaching screening age: a population-based longitudinal study. J Natl Cancer Inst 2021;113:863-8.
67. Knudsen AB, Rutter CM, Peterse EFP, et al. Colorectal cancer screening: an updated modeling study for the us preventive services task force. JAMA 2021;325:1998-2011.
68. Kuipers EJ, Spaander MC. Personalized screening for colorectal cancer. Nat Rev Gastroenterol Hepatol 2018;15:391-2.
69. Cenin DR, Naber SK, de Weerdt AC, et al. Cost-effectiveness of personalized screening for colorectal cancer based on polygenic risk and family history. Cancer Epidemiol Biomarkers Prev 2020;29:10-21.
70. Sekiguchi M, Igarashi A, Sakamoto T, Saito Y, Esaki M, Matsuda T. Cost-effectiveness analysis of colorectal cancer screening using colonoscopy, fecal immunochemical test, and risk score. J Gastroenterol Hepatol 2020;35:1555-61.
71. Naber SK, Kundu S, Kuntz KM, et al. Cost-effectiveness of risk-stratified colorectal cancer screening based on polygenic risk: current status and future potential. JNCI Cancer Spectr 2020;4:pkz086.
72. Schmidt A, Beyna T, Schumacher B, et al. Colonoscopic full-thickness resection using an over-the-scope device: a prospective multicentre study in various indications. Gut 2018;67:1280-9.
Cite This Article
Export citation file: BibTeX | RIS
OAE Style
Hsu WF, Chiu HM. Cost-effectiveness of colonoscopy and related procedures: population screening perspectives. Mini-invasive Surg 2022;6:26. http://dx.doi.org/10.20517/2574-1225.2022.03
AMA Style
Hsu WF, Chiu HM. Cost-effectiveness of colonoscopy and related procedures: population screening perspectives. Mini-invasive Surgery. 2022; 6: 26. http://dx.doi.org/10.20517/2574-1225.2022.03
Chicago/Turabian Style
Hsu, Wen-Feng, Han-Mo Chiu. 2022. "Cost-effectiveness of colonoscopy and related procedures: population screening perspectives" Mini-invasive Surgery. 6: 26. http://dx.doi.org/10.20517/2574-1225.2022.03
ACS Style
Hsu, W.F.; Chiu H.M. Cost-effectiveness of colonoscopy and related procedures: population screening perspectives. Mini-invasive. Surg. 2022, 6, 26. http://dx.doi.org/10.20517/2574-1225.2022.03
About This Article
Copyright

Data & Comments
Data
0

 Cite This Article 8 clicks
Cite This Article 8 clicks

 Like This Article 0
likes
Like This Article 0
likes






Comments
Comments must be written in English. Spam, offensive content, impersonation, and private information will not be permitted. If any comment is reported and identified as inappropriate content by OAE staff, the comment will be removed without notice. If you have any queries or need any help, please contact us at support@oaepublish.com.