
Expanding the therapeutic options for Zenker's diverticulum: from open diverticulectomy to transoral septoplasty
 0
0Abstract
Significant technical changes and a shift toward a transoral approach have occurred in the management of Zenker’s diverticulum over the past three decades. Transoral stapling is already an established and commonly performed procedure. Zenker peroral endoscopic myotomy (Z-POEM) and Zenker peroral endoscopy septotomy (Z-POES) are innovative techniques that are rapidly spreading and replacing more traditional therapeutic options. This review provides an overview of the current status of minimally invasive transoral management to assess whether a tailored approach is feasible and safe and may improve quality of life and reduce recurrence rates.
Keywords
INTRODUCTION
Zenker diverticulum (ZD) is an acquired mucosal pouch protruding from the Killian’s triangle. Pathogenetic factors include altered upper esophageal sphincter coordination, reduced hypopharyngeal wall compliance, and increased intrabolus pressure[1,2]. It is considered a rare disease, with an estimated prevalence of 0.11% or 2 per 100,000 persons per year, but the incidence will likely increase with the progressive population aging[3]. Common symptoms are dysphagia and regurgitation, and the most frequent complication is recurrent aspiration pneumonia[4]. It has been estimated that the ZD annual average caseload is 8.7 patients per year[5].
Historically, surgical treatment of ZD consisted of surgical resection of the pouch. Only during the last five decades has the crucial role of the cricopharyngeal muscle been recognized, and cricopharyngeal myotomy, performed either surgically or endoscopically, has become the main target of treatment. The developments of minimally invasive surgery and endoscopic technologies, including rigid and flexible endoscopy, have led to profound changes in management[6,7]. Most importantly, the recent introduction of Zenker peroral endoscopic myotomy (Z-POEM) reflects a better understanding of the pathophysiology of the disease and the need to minimize recurrence rates and improve the quality of life in these patients. In this review, we analyze the current status of minimally invasive transoral management of ZD.
EVOLUTION OF TREATMENT (1): FROM OPEN TO TRANSORAL SURGERY
Zenker diverticulum was initially treated by open surgery or rigid endoscopy, respectively, with the aim to resect the pouch or divide the septum between the esophagus and the diverticulum. Surgical procedures for ZD have been refined and progressively standardized using a stapler to reduce the incidence of leaks. Over time, the importance of adding a cricopharyngeal myotomy to surgical resection of the pouch has been recognized as a critical component of the surgical procedure to minimize leaks and reduce anatomical and symptomatic recurrences[8] [Table 1].
Outcomes of open surgical therapy for Zenker diverticulum
| Author | Year | No. patients | Complications (%) | Mortality (%) | Satisfactory results (%) | Recurrence (%) |
| Bonafede et al.[38] | 1997 | 87 | 24 | 3.5 | 78 | NR |
| Zbären et al.[39] | 1999 | 66 | 15 | 1.5 | 77 | 6 |
| Leporrier et al.[40] | 2001 | 40 | 17.5 | 0 | 92 | 0 |
| Gutschowet al.[41] | 2002 | 101 | 13 | 0 | 98 | 3.9 |
| Colombo-Benkmann et al.[42] | 2003 | 79 | 15 | 0 | 76 | 2.5 |
| Bonavina et al.[8] | 2007 | 116 | 3.4 | 0.8 | 84.2 | 1.7 |
| Lerut et al.[43] | 2008 | 289 | 8.5 | 0 | 94.2 | 0.03 |
| Rizzetto et al.[44] | 2008 | 77 | 13 | 0 | 95 | 5.2 |
| Greene et al. [45] | 2015 | 68 | NR | 0 | 69% | NR |
This has encouraged the development of minimally invasive transoral techniques to divide the common septum using mainly electrocautery or CO2 laser[9]. At the beginning of the laparoscopic era, transoral stapling revolutionized the therapeutic approach to ZD. The procedure, first proposed by Collard[10], Martin-Hirsch[11], and Narne[12] in 1993, consisted of division of the septum by an endoscopic linear endostapler introduced through a rigid Weerda diverticuloscope under general anesthesia. This technique showed excellent clinical outcomes, especially in patients with large-sized (> 3 cm) diverticula [Table 2]. In addition, restoration of pharyngoesophageal physiology was shown by manometric and scintigraphic studies showing decreased hypopharyngeal intrabolus pressure and improved upper esophageal sphincter clearance[13]. However, placement of the rigid diverticuloscope and actioning of the endostapler might be difficult in patients with neck stiffness or limited mouth opening[14]. In addition, the procedure is not indicated in patients with small diverticula (< 3 cm) because of the inability to engage enough cricopharyngeal muscle tissue for stapling over the entire length of the septum[15,16]. A multicenter study from the UK on 585 patients operated by otolaryngologists showed a conversion rate of 7.7%, an overall complication rate of 9.6%, and a recurrence rate of 12.8%[17]. Over the years, a modified endostapling technique using a traction suture on the apex of the septum was proposed to add an average of 1 cm of septum length into the stapler jaws, thus enabling extended septal division[18,19] [Figure 1]. In addition, various cutting and coagulation devices, including Harmonic scalpel and LigaSure, were introduced to provide complete septum division at least 1 cm distal to the uncut suture line. Soft overtubes have also been proposed to obviate the difficulties in positioning the rigid diverticuloscope[20].
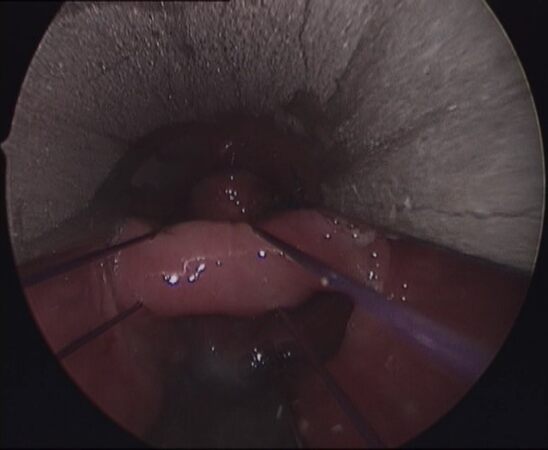
Figure 1. Transoral septum stapling: Traction sutures applied with Endostitch™ to enable extended septum division.
Outcomes of transoral stapling for Zenker diverticulum
| Author | Year | No. patients | Complications (%) | Mortality (%) | Satisfactory results (%) | Recurrence (%) |
| Cook et al.[46] | 2000 | 74 | 5 | 0 | 71 | 8.7 |
| Jaramillo et al.[47] | 2001 | 32 | 3.7 | 0 | 80 | 7.4 |
| Stoeckli et al.[48] | 2002 | 30 | 27 | 0 | 96 | NR |
| Counter et al.[49] | 2002 | 31 | 9.7 | 0 | 50 | 22 |
| Chang et al.[50] | 2003 | 150 | 12.7 | 0 | 73.3 | 11.8 |
| Wasserzug et al.[51] | 2010 | 55 | 4 | 0 | 90 | 10 |
| Bonavina et al.[52] | 2015 | 100 | 2 | 0 | 84 | 24 |
EVOLUTION OF TREATMENT (2): FROM STANDARD FLEXIBLE ENDOSCOPY TO THIRD-SPACE ENDOSCOPY
Although transoral stapling has been the preferred initial approach for ZD, lack of expertise with the rigid transoral approach, anatomic limitations of septum exposure such as reduced neck extension or inadequate mouth opening, and the requirement for narcosis have encouraged the development of flexible endoscopic techniques. Flexible endoscopic septotomy (FES) has quickly gained popularity since the first report by Ishioka et al. in 1995. Since then, this procedure has commonly been performed under deep sedation and in the outpatient setting, thus allowing the treatment of elderly patients with small (< 3 cm) pouches who may be unfit for general anesthesia[21]. Over time, different devices, such as needle-knife, hook-knife, harmonic scalpel, thulium laser, etc., have been introduced to assist the FES with satisfactory outcomes. Additionally, the use of CO2 insufflation and routine mucosal closure have consistently been recommended to minimize the risk of perforation. Regardless of the device used, FES has proven feasible and effective during
Experience with the use of POEM for esophageal achalasia[27] helped translate the principles of third-space endoscopy to the pharyngoesophageal area, thereby pushing the boundaries of FES. The Z-POEM technique has quickly gained popularity and will be accepted as the gold standard flexible endoscopic technique. Z-POEM is an innovative technique that allows cricopharyngeal myotomy through submucosal tunneling. The majority of reports now differentiate between two different tunneling techniques based on the site of mucosal incision. In the conventional technique, originally described by Li et al., the hypopharyngeal mucosa is opened 1.5-2 cm proximal to the septum and the submucosal tunneling is created to reach and divide the cricopharyngeal muscle[28]. The mucosal entry site is then closed using endoscopic clips. Performing the incision proximal to the septum makes the procedure safer, given its distance from the mediastinum, but care must be taken to avoid tearing the thin hypopharyngeal mucosa during clip closure. A limitation of Z-POEM is that only the cricopharyngeal muscle is divided, not the proximal esophageal muscle, and that the defunctionalized remnant pouch may be responsible for residual symptoms.
An alternative third-space approach, called Zenker peroral endoscopic septotomy (Z-POES), was described by Mavrogenis et al. to overcome the technical challenges of the Z-POEM technique and to improve outcomes[29]. Z-POES is a modified tunneling technique that consists in opening the mucosa alongside the long axis of the septum, directly on top of it, to gain direct access to the muscle. Then, the submucosal tunnel ahead and behind the cricopharyngeal muscle is created, and the proximal esophageal muscle fibers are also divided [Figure 2]. At the end of the myotomy, a remodeling V-shaped mucosal septal incision can be performed to widen the communication between the residual pouch and the esophagus, making this procedure particularly suitable for larger diverticula[30].

Figure 2. Z-POES: Mucosal incision and exposure of the cricopharyngeus (left); and visualization of the buccopharyngeal fascia after myotomy (right).
A recent pilot study by Repici et al. on 20 patients advocated the use of Z-POES for ZD > 20 mm in size[31]. The average procedural time was 13.8 min, and the technique was successful in 100% of patients. No symptomatic adverse events occurred, and the one-year clinical success rate was 95%. In a recent systematic review by Spadaccini et al., which included nine studies with a total of 196 patients undergoing Z-POEM or Z-POES, the pooled rate of clinical success and the pooled rate of adverse events were 93.4% and 4.9%, respectively[32]. No significant differences in terms of efficacy and safety were found between the two tunneling techniques. A recent meta-analysis of 11 studies[33] that included a total of 357 patients undergoing Z-POEM showed a pooled technical success of 96.3% (95%CI: 93.6%-97.9%), a pooled incidence of adverse events of 12.4% (95%CI: 9.1%-16.7%), and a clinical success rate of 93% (95%CI: 89.4%-95.4%). The pooled clinical recurrence rate was 11.2% (95%CI: 7.6%-16.2%).
CLINICAL RESULTS OF Z-POEM AND Z-POES
A summary of the outcomes of Z-POEM and Z-POES reported in the literature, including our personal experience, is presented in Table 3.
Literature review and personal experience with Z-POEM and Z-POES
| Author | Study design | Technique | No. of patients | Technical success (%) | Clinical success (%) | Adverse events (%) | Follow-up range, months |
| Maydeo et al., 2019[53] | Retrospective single-center | Z-POEM | 20 | 100 | 86 | No serious AE | 0-12 |
| Kamal et al., 2020[54] | Meta-analysis | Z-POEM | 233 | 95 | NR | 6 | NR |
| Yang et al., 2020[55] | Retrospective multicenter | Z-POEM | 75 | 97.3 | 92 | 6.7 (1 bleeding, 4 perforations) | 3.4-14.5 |
| Sanaei et al., 2020[56] | Retrospective multicenter | Z-POEM | 32 | 93.8 | 96 | 12.5 (2 leaks) | NR |
| Al Ghamdi et al., 2020[57] | Retrospective multicenter | Z-POEM | 91 | NR | 95 | 6 | 3-7.5 |
| Repici et al., 2020[31] | Retrospective single-center | Z-POES | 20 | 100 | 95 | No serious AE | 6-20 |
| Klingler et al., 2020[58] | Retrospective single-center | Z-POES | 19 | 94.7 | 89.5 | 10.5 (2 perforations,1 retropharyngeal abscess) | 4.7-15.5 |
| Spadaccini et al., 2021[32] | Systematic review | Z-POEM, Z-POES | 196 | 96.9 | 93.4 | 4.9 | NR |
| Personal experience [University of Milan, IRCCS Policlinico San Donato] | Retrospective single-center | Z-POES | 17 | 100 | 94.2 | 5.8 (1 leak) | 3-41 |
Over the past two decades, a total of 271 patients have been treated for ZD at our esophageal center. Of these individuals, 20 (7.4%) underwent open surgery and 198 (73%) transoral stapling through rigid endoscopy. Overall, 53 (19.6%) patients underwent a flexible endoscopic procedure, 17 (32%) of whom were treated with Z-POES. The technical success rate of the procedure was 100%, and the clinical success rate was 94.2%. One patient developed a subclinical leak which was treated conservatively with antibiotics and
DISCUSSION
The development of transoral techniques has allowed a minimally invasive and precise approach to treating ZD. However, anatomical characteristics of patients, small pouches, and lack of physician’s expertise with rigid endoscopy represent limitations of the transoral stapling technique[34]. Both Z-POEM and Z-POES appear safe and effective and may prove superior to the standard flexible endoscopy technique because they provide direct exposure of the cricopharyngeal muscle and allow performing single-stage cricopharyngeal myotomy with pouch remodeling. This may translate into a reduction of anatomical and symptomatic recurrences and lower reintervention rates.
A complete cricopharyngeal myotomy is the cornerstone of both surgical and endoscopic approaches. From the flexible endoscopic perspective, the buccopharyngeal fascia represents an important safety landmark. This thin structure is displaced posteriorly by the diverticulum, and its preservation may guarantee a complete myotomy without risks. However, it must be kept in mind that the cricopharyngeus is a circular muscle lacking an external layer of longitudinal muscle and perforation of the buccopharyngeal fascia may result in mediastinitis[35]. In real-world practice, it is challenging to identify a precise visual cue confirming that the myotomy is complete without breaking the fascia and entering the prevertebral space. Often, the trade-off to minimize the risk of perforation during standard FES is to plan a multi-stage procedure. With Z-POEM, identification of the buccopharyngeal fascia at the bottom of the pouch remains difficult during submucosal tunneling, but avoiding the posterior approach may further reduce the risk of perforation[36].
Management of ZD requires an interdisciplinary and cooperative approach. Multiple specialists (surgeons, gastroenterologists, and otolaryngologists) may be involved in the decision-making process to deliver the best care to the patient. Nowadays, indications for an open surgical approach have become rare. In our opinion, large ZD (> 3 cm) can be safely treated with endostapling, while smaller ZD can be treated with FES or Z-POES. Recurrent ZD can be safely treated with either transoral or open approach[37].
CONCLUSIONS
Peroral endoscopic myotomy techniques have opened a new era in the management of patients with ZD. However, appropriate training in advanced operative endoscopy remains critical, and high-quality studies with long-term and standardized patient-reported outcomes are necessary to validate these promising clinical findings.
DECLARATIONS
Authors’ contributionsMade substantial contributions to the conception and design of the study and performed data analysis and interpretation: Siboni S, Bonavina L
Performed data acquisition: Milito P, Scardino A
Availability of data and materialsNot applicable.
Financial support and sponsorshipNone.
Conflicts of interestAll authors declared that there are no conflicts of interest.
Ethical approval and consent to participateNot applicable.
Consent for publicationNot applicable.
Copyright© The Author(s) 2022.
REFERENCES
1. Bonavina L, Khan NA, DeMeester TR. Pharyngoesophageal dysfunctions. The role of cricopharyngeal myotomy. Arch Surg 1985;120:541-9.
2. Cook IJ, Gabb M, Panagopoulos V, et al. Pharyngeal (Zenker’s) diverticulum is a disorder of upper esophageal sphincter opening. Gastroenterology 1992;103:1229-35.
3. Law R, Katzka DA, Baron TH. Zenker’s diverticulum. Clin Gastroenterol Hepatol 2014;12:1773-82; quiz e111.
4. Siboni S, Asti E, Sozzi M, Bonitta G, Melloni M, Bonavina L. Respiratory symptoms and complications of Zenker diverticulum: effect of trans-oral septum stapling. J Gastrointest Surg 2017;21:1391-5.
5. Nitschke P, Kemper M, König P, et al. Interdisciplinary comparison of endoscopic laser-assisted diverticulotomy vs. transcervical myotomy as a treatment for Zenker’s diverticulum. J Gastrointest Surg 2020;24:1955-61.
6. Aiolfi A, Scolari F, Saino G, Bonavina L. Current status of minimally invasive endoscopic management for Zenker diverticulum. World J Gastrointest Endosc 2015;7:87-93.
7. Pescarus R, Shlomovitz E, Sharata AM, et al. Trans-oral cricomyotomy using a flexible endoscope: technique and clinical outcomes. Surg Endosc 2016;30:1784-9.
8. Bonavina L, Bona D, Abraham M, Saino G, Abate E. Long-term results of endosurgical and open surgical approach for Zenker diverticulum. World J Gastroenterol 2007;13:2586-9.
9. Overbeek JJ. Pathogenesis and methods of treatment of Zenker’s diverticulum. Ann Otol Rhinol Laryngol 2003;112:583-93.
10. Collard J, Otte J, Kestens PJ. Endoscopic stapling technique of esophagodiverticulostomy for Zenker’s diverticulum. Ann Thor Surg 1993;56:573-6.
11. Martin-Hirsch DP, Newbegin CJ. Autosuture GIA gun: a new application in the treatment of hypopharyngeal diverticula. J Laryngol Otol 1993;107:723-5.
12. Narne S, Bonavina L, Guido E, Peracchia A. Treatment of Zenker’s diverticulum by endoscopic stapling. Endosurgery 1993;1:118-20.
13. Peracchia A, Bonavina L, Narne S, Segalin A, Antoniazzi L, Marotta G. Minimally invasive surgery for Zenker diverticulum: analysis of results in 95 consecutive patients. Arch Surg 1998;133:695-700.
14. Bloom JD, Bleier BS, Mirza N, Chalian AA, Thaler ER. Factors predicting endoscopic exposure of Zenker’s diverticulum. Ann Otol Rhinol Laryngol 2010;119:736-41.
15. Narne S, Cutrone C, Bonavina L, Chella B, Peracchia A. Endoscopic diverticulotomy for the treatment of Zenker’s diverticulum: results in 102 patients with staple-assisted endoscopy. Ann Otol Rhinol Laryngol 1999;108:810-5.
16. Tsikoudas A, Eason D, Kara N, Brunton JN, Mountain RE. Correlation of radiologic findings and clinical outcome in pharyngeal pouch stapling. Ann Otol Rhinol Laryngol 2006;115:721-6.
17. Leong SC, Wilkie MD, Webb CJ. Endoscopic stapling of Zenker’s diverticulum: establishing national baselines for auditing clinical outcomes in the United Kingdom. Eur Arch Otorhinolaryngol 2012;269:1877-84.
18. Nicholas BD, Devitt S, Rosen D, Spiegel J, Boon M. Endostitch-assisted endoscopic Zenker’s diverticulostomy: a tried approach for difficult cases. Dis Esophagus 2010;23:296-9.
19. Bonavina L, Rottoli M, Bona D, Siboni S, Russo IS, Bernardi D. Transoral stapling for Zenker diverticulum: effect of the traction suture-assisted technique on long-term outcomes. Surg Endosc 2012;26:2856-61.
20. Bonavina L, Bona D, Aiolfi A, Sironi A. Transoral septum stapling of Zenker diverticulum is feasible and safe through a soft overtube. Surg Innov 2015;22:207-9.
21. Ishioka S, Sakai P, Maluf Filho F, Melo JM. Endoscopic incision of Zenker’s diverticula. Endoscopy 1995;27:433-7.
22. Bizzotto A, Iacopini F, Landi R, Costamagna G. Zenker’s diverticulum: exploring treatment options. Acta Otorhinolaryngol Ital 2013;33:219-29.
23. Zanghì S, Siboni S, Asti E, Bonavina L. Endoscopic stapling versus laser for Zenker diverticulum: a retrospective cohort study. Eur Arch Otorhinolaryngol 2021;278:2625-30.
24. Ishaq S, Hassan C, Antonello A, et al. Flexible endoscopic treatment for Zenker’s diverticulum: a systematic review and meta-analysis. Gastrointest Endosc 2016;83:1076-1089.e5.
25. Verdonck J, Morton RP. Systematic review on treatment of Zenker’s diverticulum. Eur Arch Otorhinolaryngol 2015;272:3095-107.
26. Bhatt NK, Mendoza J, Kallogjeri D, Hardi AC, Bradley JP. Comparison of surgical treatments for zenker diverticulum: a systematic review and network meta-analysis. JAMA Otolaryngol Head Neck Surg 2021;147:190-6.
27. Lois AW, Oelschlager BK, Wright AS, Templeton AW, Flum DR, Farjah F. Use and safety of per-oral endoscopic myotomy for achalasia in the US. JAMA Surg 2022;157:490-7.
28. Li QL, Chen WF, Zhang XC, et al. Submucosal tunneling endoscopic septum division: a novel technique for treating Zenker’s diverticulum. Gastroenterology 2016;151:1071-4.
29. Mavrogenis G, Tsevgas I, Zachariadis D, Bazerbachi F. Mucosotomy at the top of the septum facilitates tunneling and clipping during peroral endoscopic myotomy for Zenker’s diverticulum (Z-POEM). Ann Gastroenterol 2020;33:101.
30. Zhang LY, Nieto J, Ngamruengphong S, Repici A, Khashab MA. Zenker’s diverticulum: advancing beyond the tunnel. VideoGIE 2021;6:562-7.
31. Repici A, Spadaccini M, Belletrutti PJ, et al. Peroral endoscopic septotomy for short-septum Zenker’s diverticulum. Endoscopy 2020;52:563-8.
32. Spadaccini M, Maselli R, Chandrasekar VT, et al. Submucosal tunnelling techniques for Zenker’s diverticulum: a systematic review of early outcomes with pooled analysis. Eur J Gastroenterol Hepatol 2021;33:e78-83.
33. Zhang H, Huang S, Xia H, et al. The role of peroral endoscopic myotomy for Zenker’s diverticulum: a systematic review and meta-analysis. Surg Endosc 2022;36:2749-59.
34. Milito P, Siboni S, Asti E, Bonavina L. Anthropometric variables predict feasibility and long-term outcomes of trans-oral septum stapling for Zenker diverticulum. J Gastrointest Surg 2022; doi: 10.1007/s11605-022-05432-8.
35. Ishaq S, Kuwai T, Siau K, Mulder CJ, Neumann H. Is Z-POEM for Zenker’s the same as POEM for achalasia? Gastrointest Endosc 2020;91:204-5.
36. Chang CW, Liou SS, Netterville JL. Anatomic study of laser-assisted endoscopic cricopharyngeus myotomy. Ann Otol Rhinol Laryngol 2005;114:897-901.
37. Berger MH, Weiland D, Tierney WS, et al. Surgical management of recurrent Zenker’s diverticulum: a multi-institutional cohort study. Am J Otolaryngol 2021;42:102755.
38. Bonafede JP, Lavertu P, Wood BG, Eliachar I. Surgical outcome in 87 patients with Zenker’s diverticulum. Laryngoscope 1997;107:720-5.
39. Zbären P, Schär P, Tschopp L, Becker M, Häusler R. Surgical treatment of Zenker’s diverticulum: transcutaneous diverticulectomy versus microendoscopic myotomy of the cricopharyngeal muscle with CO2 laser. Otolaryngol Head Neck Surg 1999;121:482-7.
40. Leporrier J, Salamé E, Gignoux M, Ségol P. Diverticule de Zenker: diverticulopexie contre diverticulectomie. Annales de Chirurgie 2001;126:42-5.
41. Gutschow CA, Hamoir M, Rombaux P, Otte J, Goncette L, Collard J. Management of pharyngoesophageal (Zenker’s) diverticulum: which technique? Ann Thor Surg 2002;74:1677-83.
42. Colombo-benkmann M, Unruh V, Krieglstein C, Senninger N. Cricopharyngeal myotomy in the treatment of Zenker’s diverticulum. J Am College Surg 2003;196:370-7.
43. Lerut T, van Raemdonck D, Guelinckx P, Dom R, Geboes K. Zenker’s diverticulum: is a myotomy of the cricopharyngeus useful? Hepatogastroenterology 1992;39:127-31.
44. Rizzetto C, Zaninotto G, Costantini M, et al. Zenker’s diverticula: feasibility of a tailored approach based on diverticulum size. J Gastrointest Surg 2008;12:2057-64; discussion 2064.
45. Greene CL, McFadden PM, Oh DS, Chang EJ, Hagen JA. Long-term outcome of the treatment of Zenker’S diverticulum. Ann Thorac Surg 2015;100:975-8.
46. Cook RD, Huang PC, Richstmeier WJ, Scher RL. Endoscopic staple-assisted esophagodiverticulostomy: an excellent treatment of choice for Zenker’s diverticulum. Laryngoscope 2000;110:2020-5.
47. Jaramillo MJ, McLay KA, McAteer D. Long-term clinico-radiological assessment of endoscopic stapling of pharyngeal pouch: a series of cases. J Laryngol Otol 2001;115:462-6.
48. Stoeckli SJ, Schmid S. Endoscopic stapler-assisted diverticuloesophagostomy for Zenker’s diverticulum: patient satisfaction and subjective relief of symptoms. Surgery 2002;131:158-62.
49. Counter PR, Hilton ML, Baldwin DL. Long-term follow-up of endoscopic stapled diverticulotomy. Ann R Coll Surg Engl 2002;84:89-92.
50. Chang CW, Burkey BB, Netterville JL, Courey MS, Garrett CG, Bayles SW. Carbon dioxide laser endoscopic diverticulotomy versus open diverticulectomy for Zenker’s diverticulum. Laryngoscope 2004;114:519-27.
51. Wasserzug O, Zikk D, Raziel A, Cavel O, Fleece D, Szold A. Endoscopically stapled diverticulostomy for Zenker’s diverticulum: results of a multidisciplinary team approach. Surg Endosc 2010;24:637-41.
52. Bonavina L, Aiolfi A, Scolari F, Bona D, Lovece A, Asti E. Long-term outcome and quality of life after transoral stapling for Zenker diverticulum. World J Gastroenterol 2015;21:1167-72.
53. Maydeo A, Patil GK, Dalal A. Operative technical tricks and 12-month outcomes of diverticular peroral endoscopic myotomy (D-POEM) in patients with symptomatic esophageal diverticula. Endoscopy 2019;51:1136-40.
54. Kamal F, Khan MA, Lee-Smith W, et al. Peroral endoscopic myotomy is a safe and feasible option in management of esophageal diverticula: systematic review and meta-analysis. Dig Dis Sci 2021;66:3242-9.
55. Yang J, Novak S, Ujiki M, et al. An international study on the use of peroral endoscopic myotomy in the management of Zenker’s diverticulum. Gastrointest Endosc 2020;91:163-8.
56. Sanaei O, Ichkhanian Y, Mondragón OVH, et al. Impact of prior treatment on feasibility and outcomes of Zenker’s peroral endoscopic myotomy (Z-POEM). Endoscopy 2021;53:722-6.
57. Al Ghamdi SS, Farha J, Meybodi MA, et al. 51 international multicenter study comparing z-poem and flexible/rigid endoscopic Zenker’S diverticulotomy. Gastro Endosc 2020;91:AB3-4.
Cite This Article
Export citation file: BibTeX | RIS
OAE Style
Scardino A, Siboni S, Milito P, Bonavina L. Expanding the therapeutic options for Zenker's diverticulum: from open diverticulectomy to transoral septoplasty. Mini-invasive Surg 2022;6:57. http://dx.doi.org/10.20517/2574-1225.2022.55
AMA Style
Scardino A, Siboni S, Milito P, Bonavina L. Expanding the therapeutic options for Zenker's diverticulum: from open diverticulectomy to transoral septoplasty. Mini-invasive Surgery. 2022; 6: 57. http://dx.doi.org/10.20517/2574-1225.2022.55
Chicago/Turabian Style
Scardino, Andrea, Stefano Siboni, Pamela Milito, Luigi Bonavina. 2022. "Expanding the therapeutic options for Zenker's diverticulum: from open diverticulectomy to transoral septoplasty" Mini-invasive Surgery. 6: 57. http://dx.doi.org/10.20517/2574-1225.2022.55
ACS Style
Scardino, A.; Siboni S.; Milito P.; Bonavina L. Expanding the therapeutic options for Zenker's diverticulum: from open diverticulectomy to transoral septoplasty. Mini-invasive. Surg. 2022, 6, 57. http://dx.doi.org/10.20517/2574-1225.2022.55
About This Article
Special Issue
Copyright

Data & Comments
Data
0

 Cite This Article 12 clicks
Cite This Article 12 clicks

 Like This Article 1
likes
Like This Article 1
likes






Comments
Comments must be written in English. Spam, offensive content, impersonation, and private information will not be permitted. If any comment is reported and identified as inappropriate content by OAE staff, the comment will be removed without notice. If you have any queries or need any help, please contact us at support@oaepublish.com.